

The Tubulointerstitial Pathophysiology of Progressive Kidney Disease
- PMID: 28284376
- PMCID: PMC5351778
- DOI: 10.1053/j.ackd.2016.11.011
The Tubulointerstitial Pathophysiology of Progressive Kidney Disease
Abstract
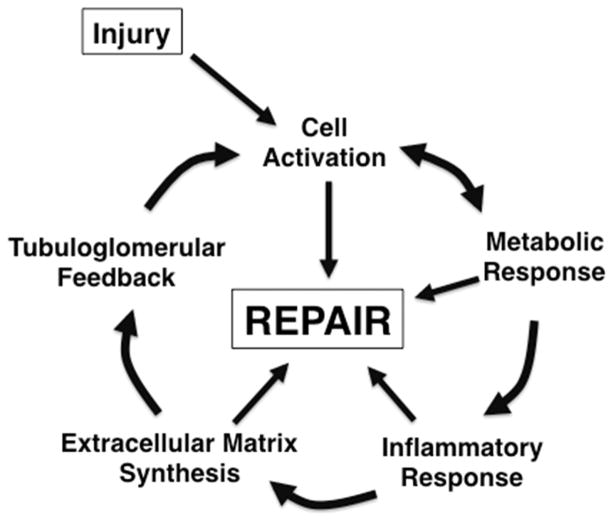
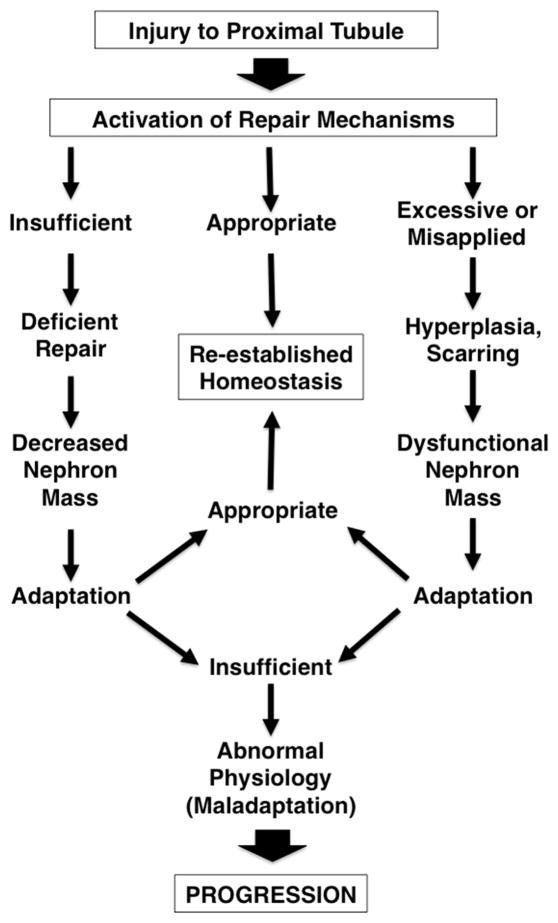
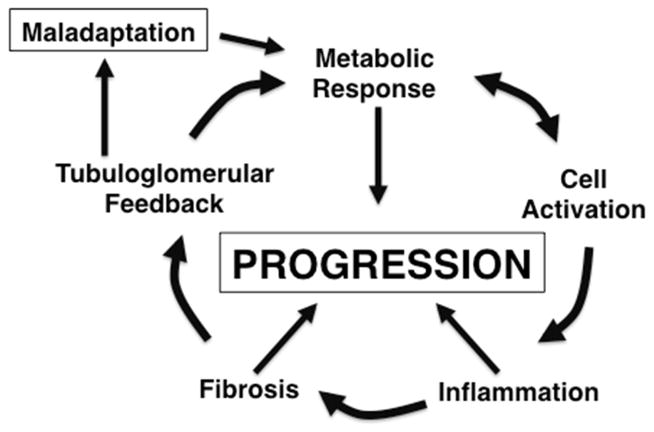
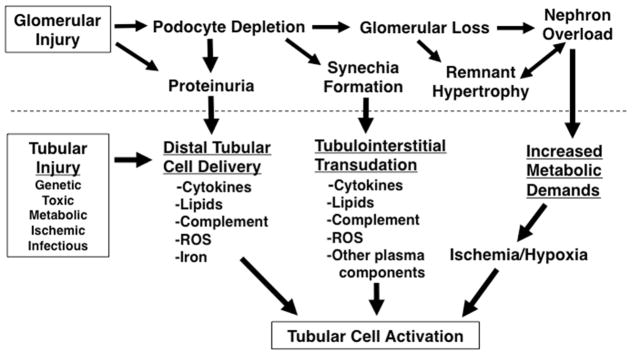
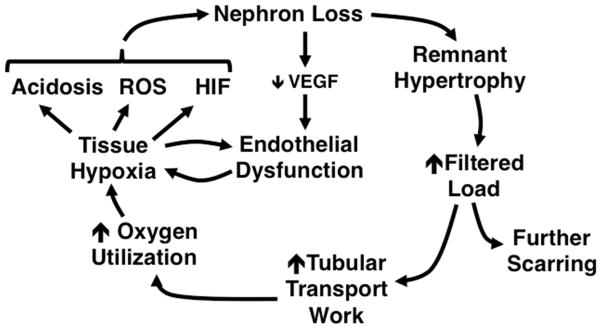
Accumulating evidence suggests that the central locus for the progression of CKD is the renal proximal tubule. As injured tubular epithelial cells dedifferentiate in attempted repair, they stimulate inflammation and recruit myofibroblasts. At the same time, tissue loss stimulates remnant nephron hypertrophy. Increased tubular transport workload eventually exceeds the energy-generating capacity of the hypertrophied nephrons, leading to anerobic metabolism, acidosis, hypoxia, endoplasmic reticulum stress, and the induction of additional inflammatory and fibrogenic responses. The result is a vicious cycle of injury, misdirected repair, maladaptive responses, and more nephron loss. Therapy that might be advantageous at one phase of this progression pathway could be deleterious during other phases. Thus, interrupting this downward spiral requires narrowly targeted approaches that promote healing and adequate function without generating further entry into the progression cycle.
Keywords: CKD; Fibrosis; Proximal tubule; Remnant nephron.
Copyright © 2016 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The author has no conflicts to disclose
Figures
References
-
- Wiggins RC. The spectrum of podocytopathies: a unifying view of glomerular diseases. Kidney international. 2007;71(12):1205–1214. - PubMed
-
- Kriz W, Gretz N, Lemley KV. Progression of glomerular diseases: is the podocyte the culprit? Kidney international. 1998;54(3):687–697. - PubMed
-
- Bonsib SM. Focal-segmental glomerulosclerosis. The relationship between tubular atrophy and segmental sclerosis. Am J Clin Pathol. 1999;111(3):343–348. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
