

Association between Off-Peak Hour Birth and Neonatal Morbidity and Mortality among Very Low Birth Weight Infants
- PMID: 28284476
- PMCID: PMC5500004
- DOI: 10.1016/j.jpeds.2017.02.007
Association between Off-Peak Hour Birth and Neonatal Morbidity and Mortality among Very Low Birth Weight Infants
Abstract
Objective: To assess the independent association between overnight or "off-peak" hour delivery and 3 neonatal morbidities strongly associated with childhood neurocognitive impairment.
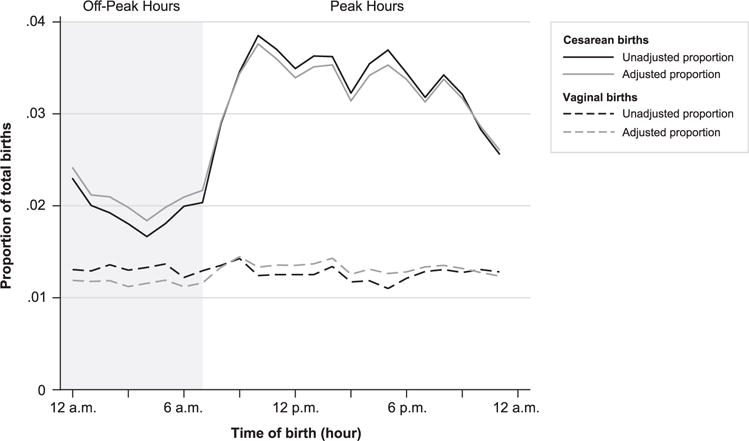
Study design: Retrospective population based cohort study of all infants with birth weights of 500-1499 g born without severe congenital anomalies in California or Pennsylvania between 2002 and 2009. Off-peak hour delivery was defined as birth between 12:00 a.m. and 6:59 a.m. The study outcomes were death; bronchopulmonary dysplasia, retinopathy of prematurity, and severe (grade 3 or 4) intraventricular hemorrhage among survivors; the composite of each morbidity or mortality; and the composite of death or 1 or more of the evaluated morbidities.
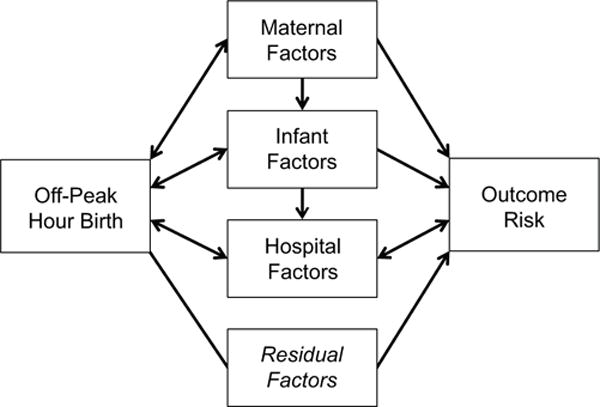
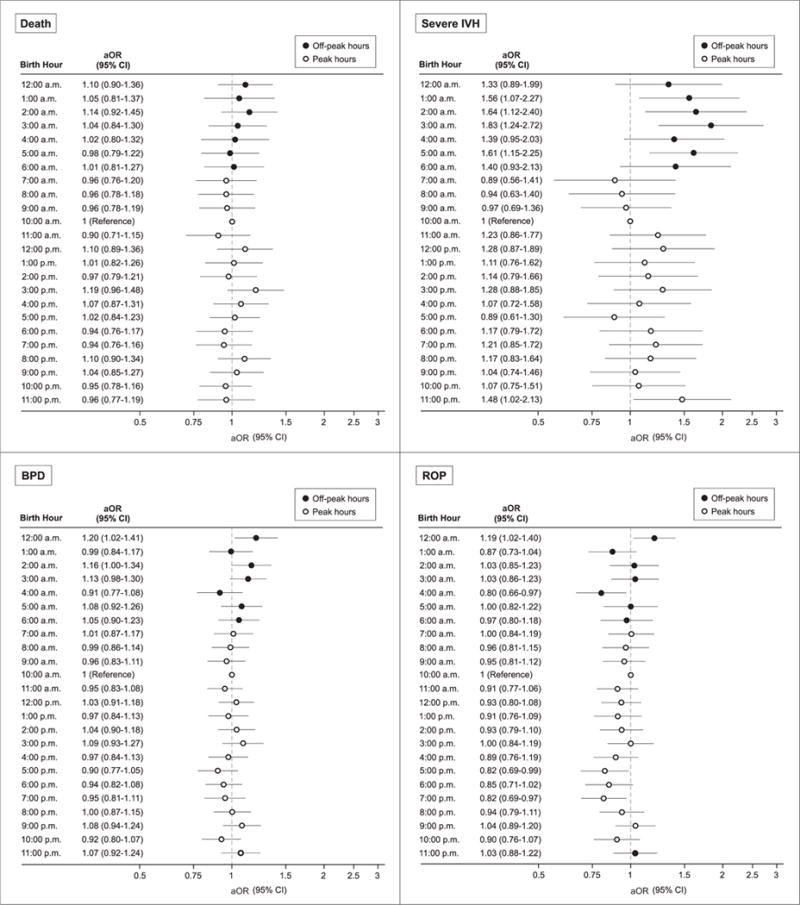
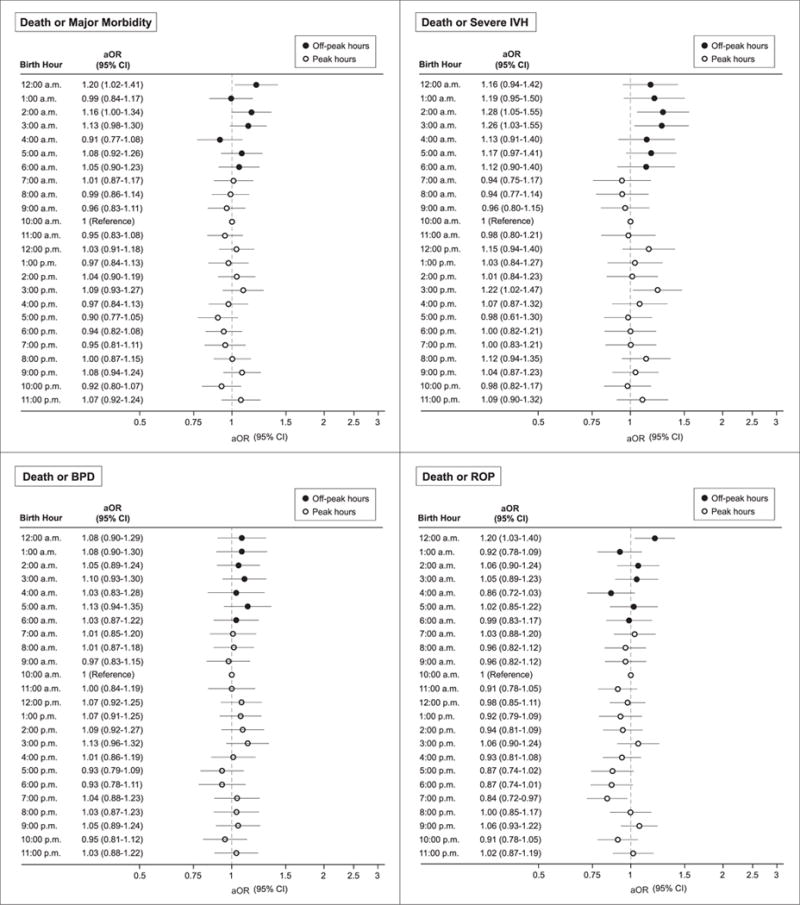
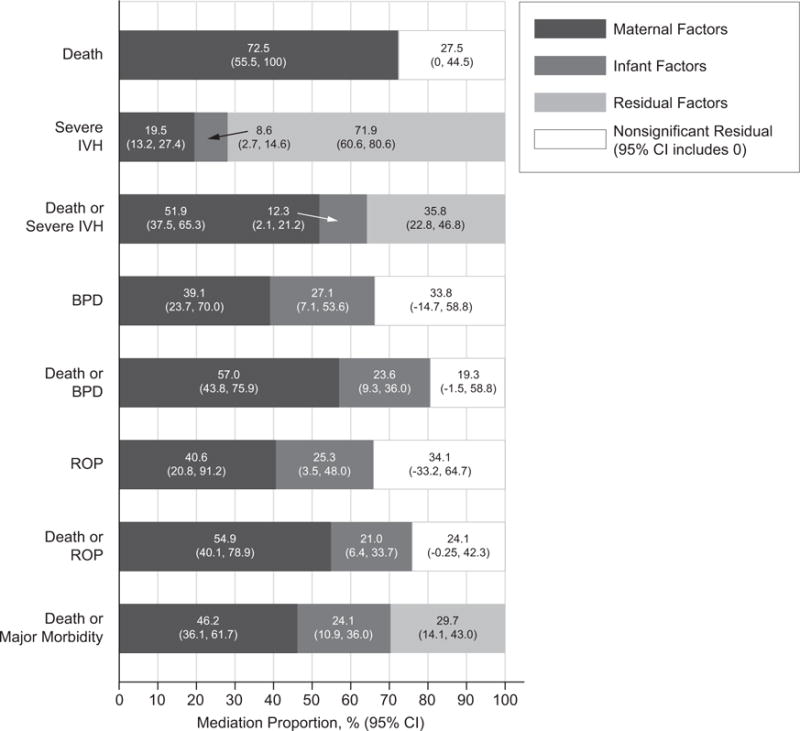
Results: Of 47 617 evaluated infants, 9317 (19.6%) were born during off-peak hours. The frequencies of all study outcomes were higher among infants born during off-peak compared with peak hours. After adjusting for maternal, infant, and hospital characteristics, off-peak hour delivery was associated with increased odds of severe intraventricular hemorrhage among survivors (OR 1.39, 95% CI 1.23-1.57) and the composite outcomes of death or severe intraventricular hemorrhage (OR 1.16, 95% CI 1.07-1.25) and death or major morbidity (OR 1.08, 95% CI 1.02-1.15). There was no evidence of subgroup effects based on delivery mode, birth hospital neonatal intensive care level or annual very low birth weight infant delivery volume, or weekday vs weekend off-peak hour delivery for any study outcome.
Conclusions: Very low birth weight infants born between midnight and 7:00 a.m. are at increased risk for severe intraventricular hemorrhage and death or major neonatal morbidity.
Keywords: bronchopulmonary dysplasia; intraventricular hemorrhage; overnight birth; retinopathy of prematurity.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Large Data and the Risks of Misleading Conclusions.J Pediatr. 2017 Jul;186:7-9. doi: 10.1016/j.jpeds.2017.03.041. Epub 2017 Apr 7. J Pediatr. 2017. PMID: 28396021 No abstract available.
References
-
- Mathew T, Curtin S. When are babies born: Morning, noon, or night? Birth certificate data for 2013. Hyattsville, MD: National Center for Health Statistics; 2015. (NCHS data brief, no 200). - PubMed
-
- Lee SK, Lee DSC, Andrews WL, Baboolal R, Pendray M, Stewart S, et al. Higher mortality rates among inborn infants admitted to neonatal intensive care units at night. J Pediatr. 2003;143:592–7. - PubMed
-
- Paccaud F, Martin-Béran B, Gutzwiller F. Hour of birth as a prognostic factor for perinatal death. Lancet. 1988;1:340–3. - PubMed
-
- Gould JB, Qin C, Chavez G. Time of birth and the risk of neonatal death. Obstet Gynecol. 2005;106:352–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
