

Time to Clinically Relevant Fracture Risk Scores in Postmenopausal Women
- PMID: 28285070
- PMCID: PMC5474146
- DOI: 10.1016/j.amjmed.2017.02.012
Time to Clinically Relevant Fracture Risk Scores in Postmenopausal Women
Abstract
Background: Clinical practice guidelines recommend use of fracture risk scores for screening and pharmacologic treatment decisions. The timing of occurrence of treatment-level (according to 2014 National Osteoporosis Foundation guidelines) or screening-level (according to 2011 US Preventive Services Task Force guidelines) fracture risk scores has not been estimated in postmenopausal women.
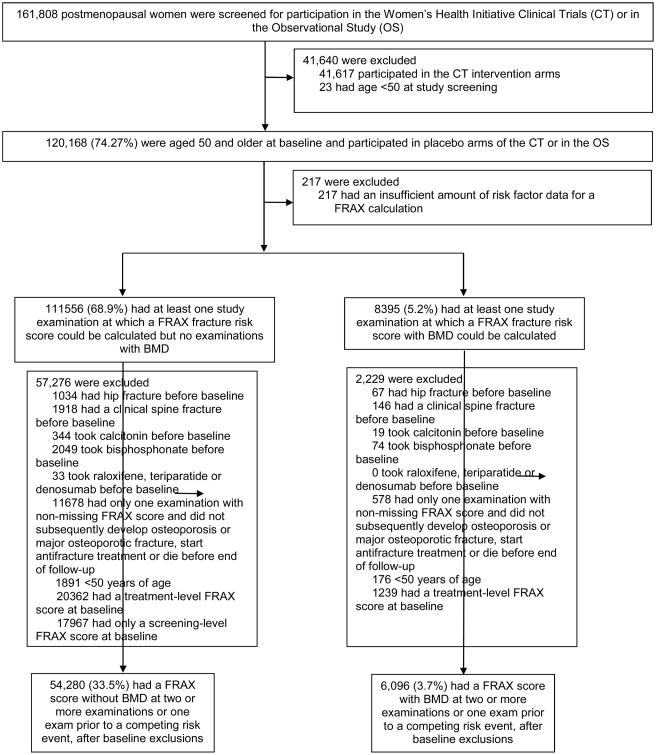
Methods: We conducted a retrospective competing risk analysis of new occurrence of treatment-level and screening-level fracture risk scores in postmenopausal women aged 50 years and older, prior to receipt of pharmacologic treatment and prior to first hip or clinical vertebral fracture.
Results: In 54,280 postmenopausal women aged 50 to 64 years without a bone mineral density test, the time for 10% to develop a treatment-level FRAX score could not be estimated accurately because of rare incidence of treatment-level scores. In 6096 women who had FRAX scores calculated with bone mineral density, the estimated unadjusted time to treatment-level FRAX ranged from 7.6 years (95% confidence interval [CI], 6.6-8.7) for those aged 65 to 69, to 5.1 years (95% CI, 3.5-7.5) for those aged 75 to 79 at baseline. Of 17,967 women aged 50 to 64 with a screening-level FRAX at baseline, 100 (0.6%) experienced a hip or clinical vertebral fracture by age 65 years.
Conclusions: Postmenopausal women with sub-threshold fracture risk scores at baseline were unlikely to develop a treatment-level FRAX score between ages 50 and 64 years. After age 65, the increased incidence of treatment-level fracture risk scores, osteoporosis, and major osteoporotic fracture supports more frequent consideration of FRAX and bone mineral density testing.
Trial registration: ClinicalTrials.gov NCT00000611.
Keywords: Bone density; Fractures; Menopausal; Osteoporosis/epidemiology; Risk assessment.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- World Health Organization Collaborating Centre for Metabolic Bone Diseases, University of Sheffield, UK. University of Sheffield; Sheffield, UK: [Accessed December 27, 2016]. FRAX: WHO Fracture Risk Assessment Tool [Internet] Available from http://www.shef.ac.uk/FRAX/
-
- Dawson-Hughes B, Tosteson AN, Melton LJ, 3rd, et al. Implications of absolute fracture risk assessment for osteoporosis practice guidelines in the USA. Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2008;19(4):449–458. - PubMed
-
- Tosteson AN, Melton LJ, 3rd, Dawson-Hughes B, et al. Cost-effective osteoporosis treatment thresholds: the United States perspective. Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2008;19(4):437–447. - PMC - PubMed
-
- Screening for osteoporosis: U.S. preventive services task force recommendation statement. Ann Intern Med. 2011;154(5):356–364. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- HHSN268201100001I/HL/NHLBI NIH HHS/United States
- R01 AG046294/AG/NIA NIH HHS/United States
- HHSN268201100004I/HL/NHLBI NIH HHS/United States
- HHSN268201100046C/HL/NHLBI NIH HHS/United States
- HHSN268201100003C/WH/WHI NIH HHS/United States
- HHSN271201100004C/AG/NIA NIH HHS/United States
- HHSN268201100002C/WH/WHI NIH HHS/United States
- UL1 TR000083/TR/NCATS NIH HHS/United States
- HHSN268201100003I/HL/NHLBI NIH HHS/United States
- HHSN268201100002I/HL/NHLBI NIH HHS/United States
- HHSN268201100001C/WH/WHI NIH HHS/United States
- HHSN268201100004C/WH/WHI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
