

A Novel Rehabilitation Intervention for Older Patients With Acute Decompensated Heart Failure: The REHAB-HF Pilot Study
- PMID: 28285121
- PMCID: PMC5409854
- DOI: 10.1016/j.jchf.2016.12.019
A Novel Rehabilitation Intervention for Older Patients With Acute Decompensated Heart Failure: The REHAB-HF Pilot Study
Abstract
Objectives: This study sought to assess a novel physical rehabilitation intervention in older patients hospitalized for acute decompensated heart failure (ADHF).
Background: After ADHF, older patients, who are frequently frail with multiple comorbidities, have prolonged and incomplete recovery of physical function and remain at high risk for poor outcomes.
Methods: The REHAB-HF (Rehabilitation Therapy in Older Acute Heart Failure Patients) pilot study was a 3-site, randomized, attention-controlled pilot study of a tailored, progressive, multidomain physical rehabilitation intervention beginning in the hospital and continuing for 12 weeks post-discharge in patients ≥60 years hospitalized with ADHF. The primary purpose was to assess the feasibility and reasonableness of the hypothesis that the novel rehabilitation intervention would improve physical function (Short Physical Performance Battery [SPPB]) over 3 months and reduce all-cause rehospitalizations over 6 months.
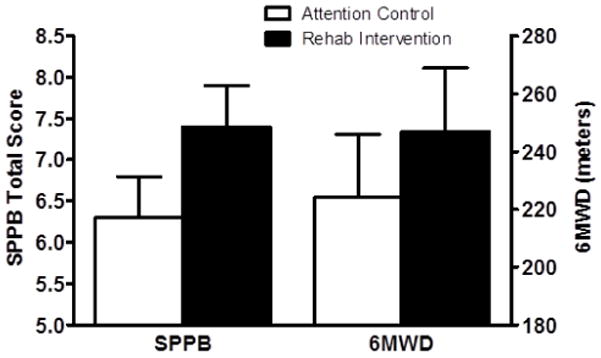
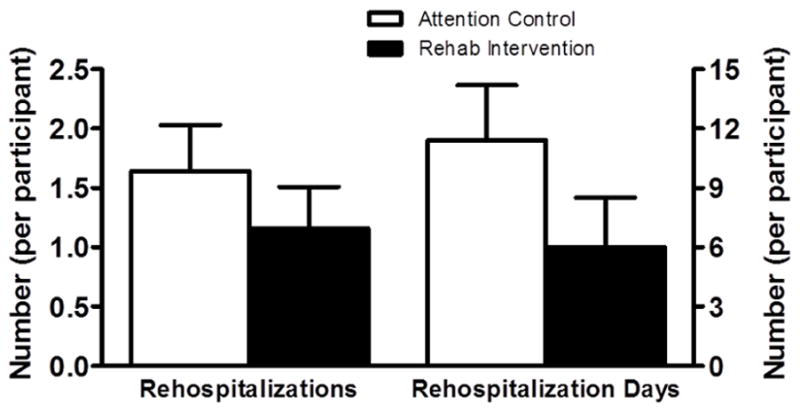
Results: The study enrolled 27 patients with ADHF (ages 60 to 98 years; 59% women; 56% African American; 41% with preserved ejection fraction [≥45%]). At baseline, participants had marked impairments in physical function, multiple comorbidities, and frailty. Study retention (89%) and intervention adherence (93%) were excellent. At 3 months, an intervention effect size was measured for the SPPB score of +1.1 U (7.4 ± 0.5 U vs. 6.3 ± 0.5 U), and at 6 months an effect size was observed for an all-cause rehospitalization rate of -0.48 (1.16 ± 0.35 vs. 1.64 ± 0.39). The change in SPPB score was strongly related to all-cause rehospitalizations, explaining 91% of change.
Conclusions: These findings support the feasibility and rationale for a recently launched, National Institutes of Health-funded trial to test the safety and efficacy of this novel multidomain physical rehabilitation intervention to improve physical function and reduce rehospitalizations in older, frail patients with ADHF with multiple comorbidities. (Rehabilitation and Exercise Training After Hospitalization [REHAB-HF]; NCT01508650; A Trial of Rehabilitation Therapy in Older Acute Heart Failure Patients [REHAB-HF]; NCT02196038).
Keywords: exercise; frailty; hospitalization; physical function; rehabilitation.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Lloyd-Jones D, Adams RJ, Brown TM, et al. Executive summary: heart disease and stroke statistics--2010 update: a report from the American Heart Association. Circulation. 2010;121:948–54. - PubMed
-
- Kociol RD, Peterson ED, Hammill BG, et al. National Survey of Hospital Strategies to Reduce Heart Failure Readmissions: Findings From the Get With the Guidelines-Heart Failure Registry. Circ Heart Fail. 2012;5:680–687. - PubMed
-
- Cheng RK, Cox M, Neely ML, et al. Outcomes in patients with heart failure with preserved, borderline, and reduced ejection fraction in the Medicare population. Am Heart J. 2014;168:721–30. - PubMed
-
- Sanchez E, Vidan MT, Serra JA, Fernandez-Aviles F, Bueno H. Prevalence of geriatric syndromes and impact on clinical and functional outcomes in older patients with acute cardiac diseases. Heart. 2011;97:1602–6. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
