

Rotational Osteotomy for Hallux Valgus. A New Technique for Primary and Revision Cases
- PMID: 28286430
- PMCID: PMC5335916
- DOI: 10.1097/BTF.0000000000000142
Rotational Osteotomy for Hallux Valgus. A New Technique for Primary and Revision Cases
Abstract
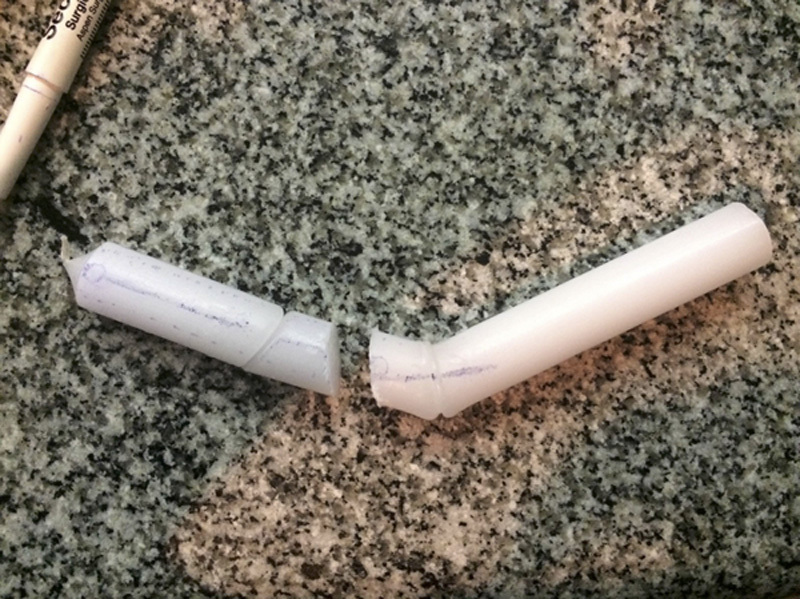
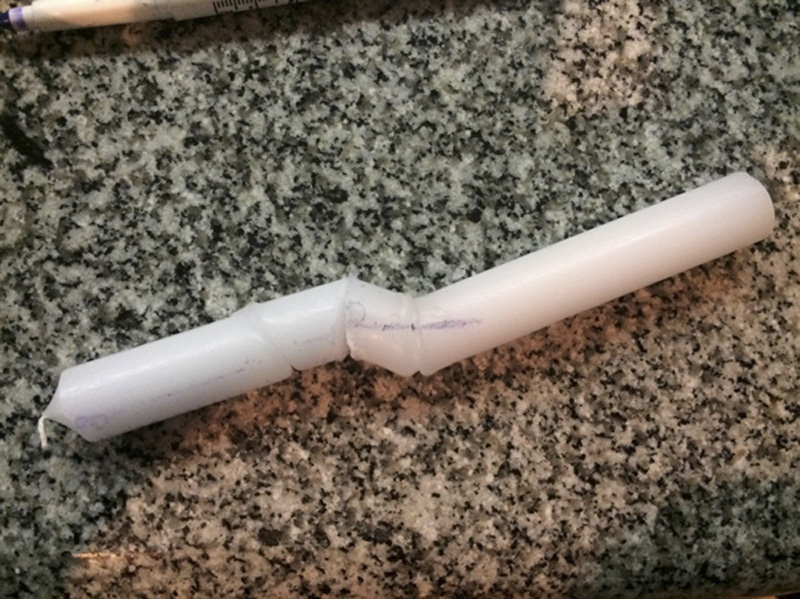
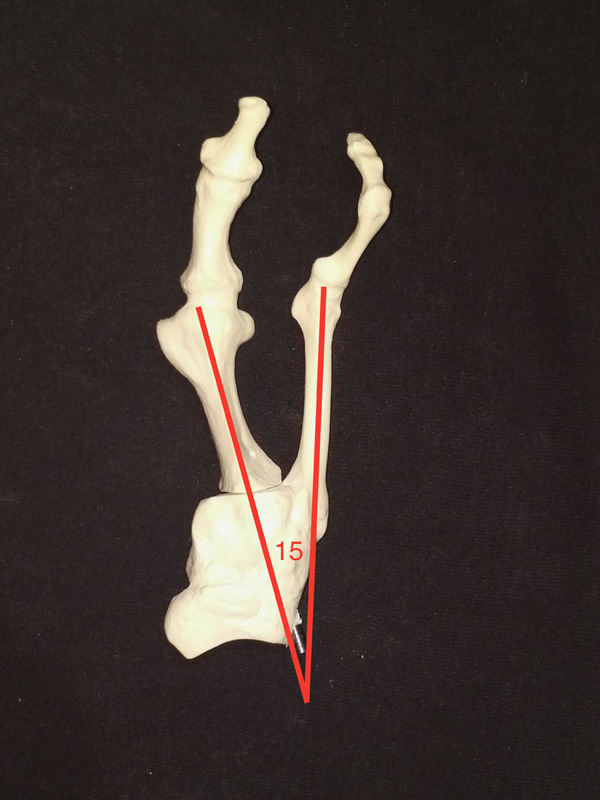
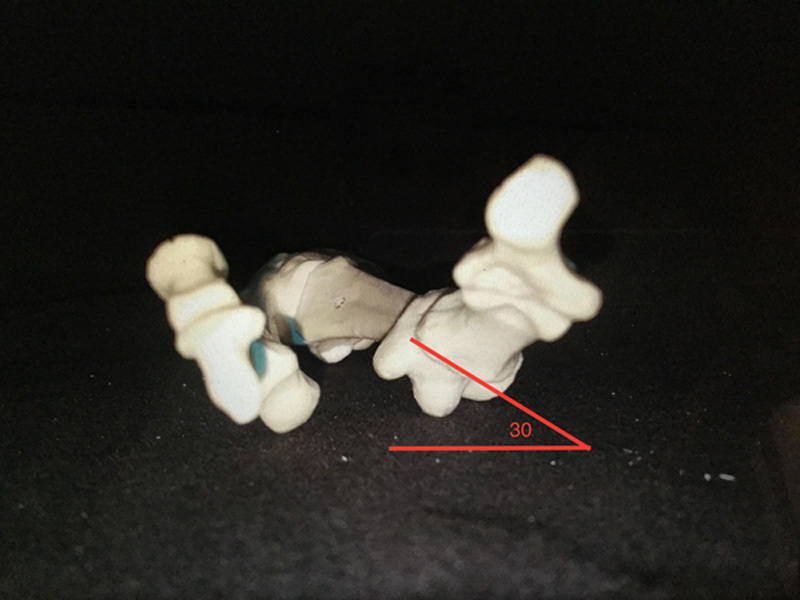
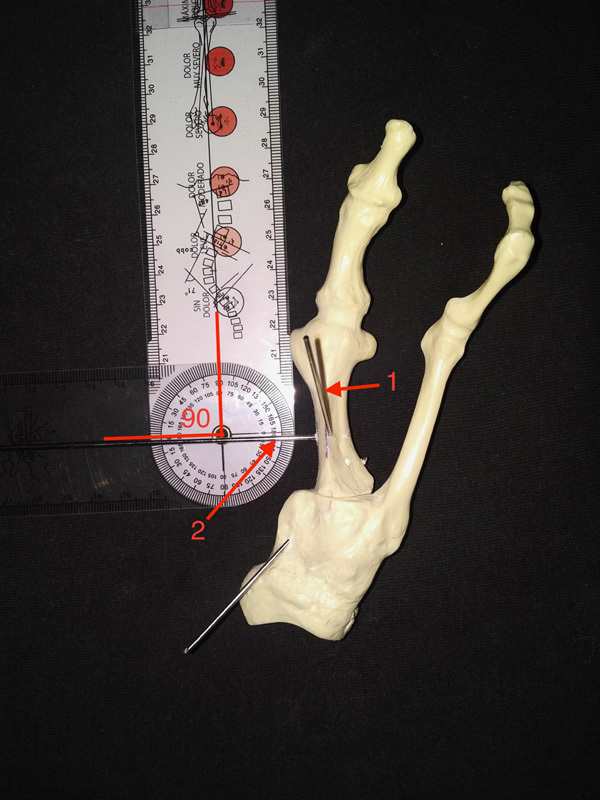
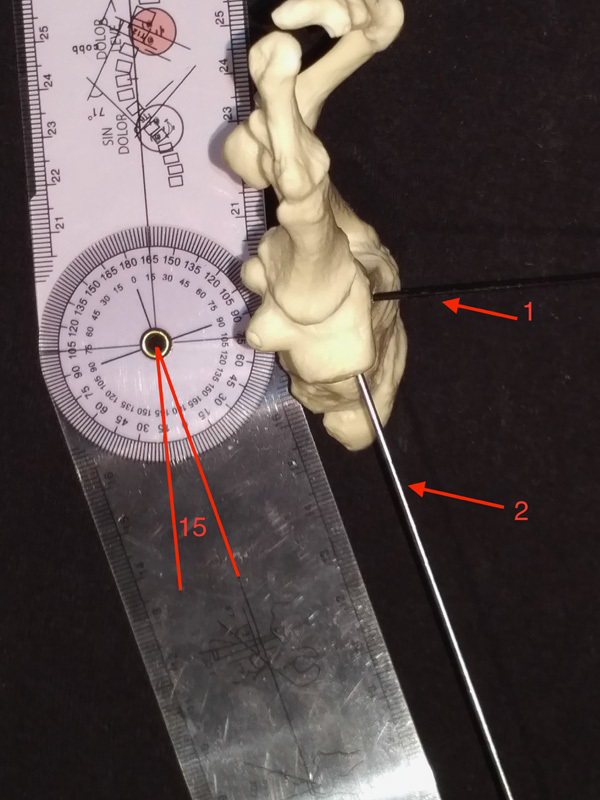
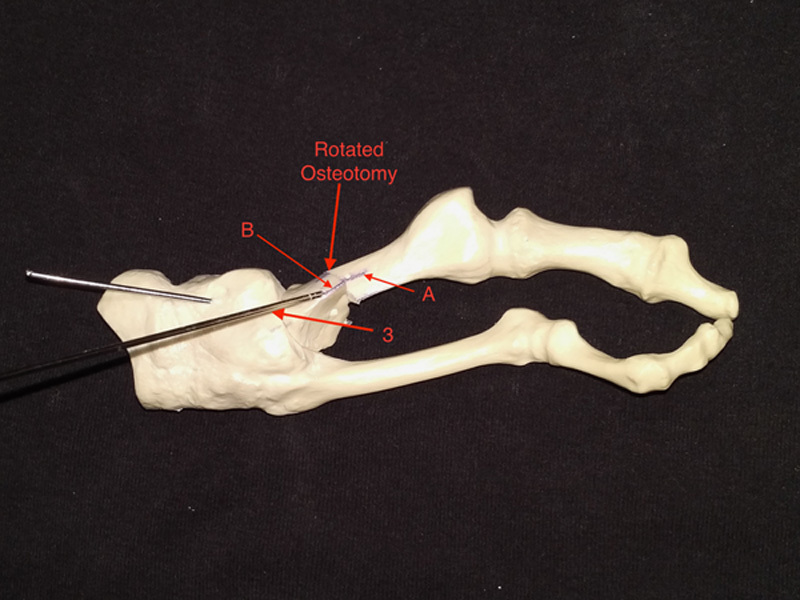
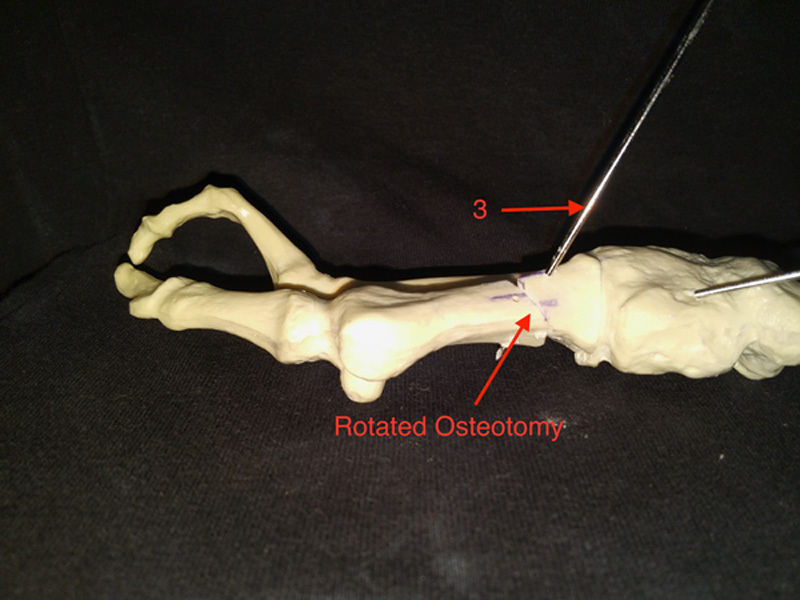
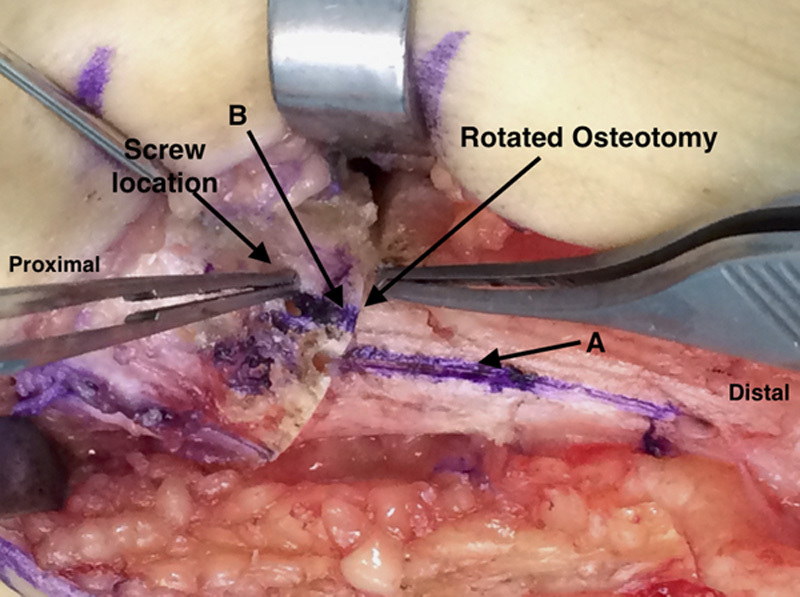
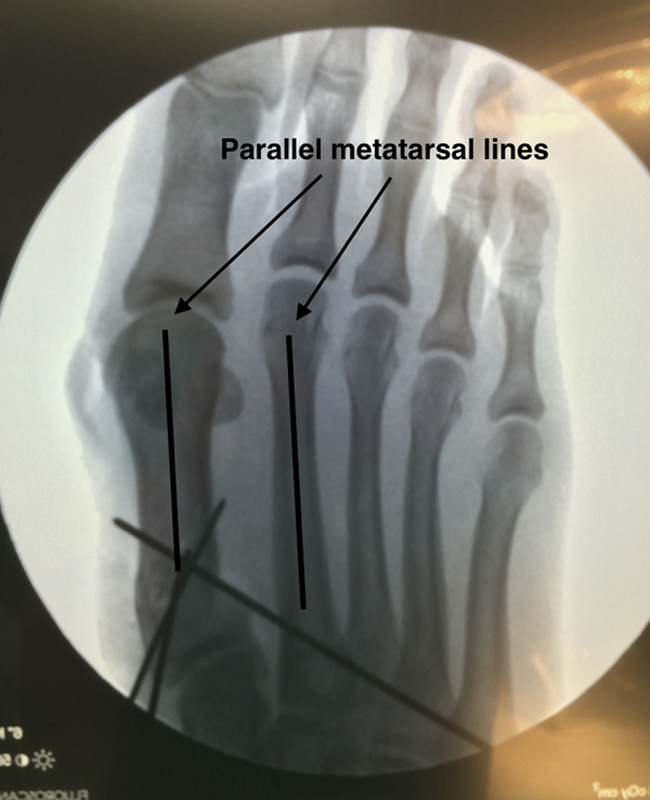
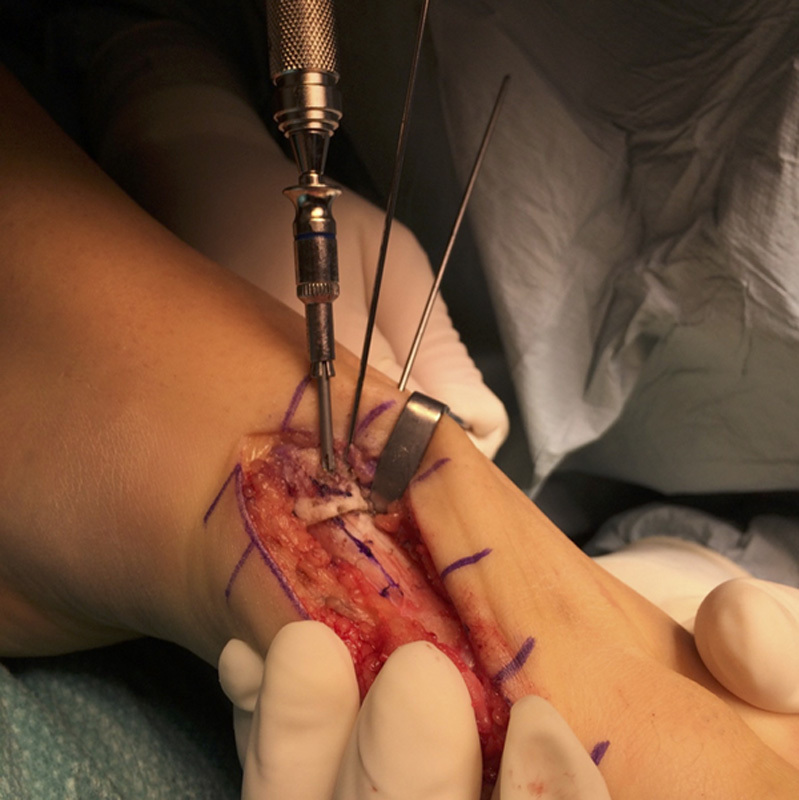
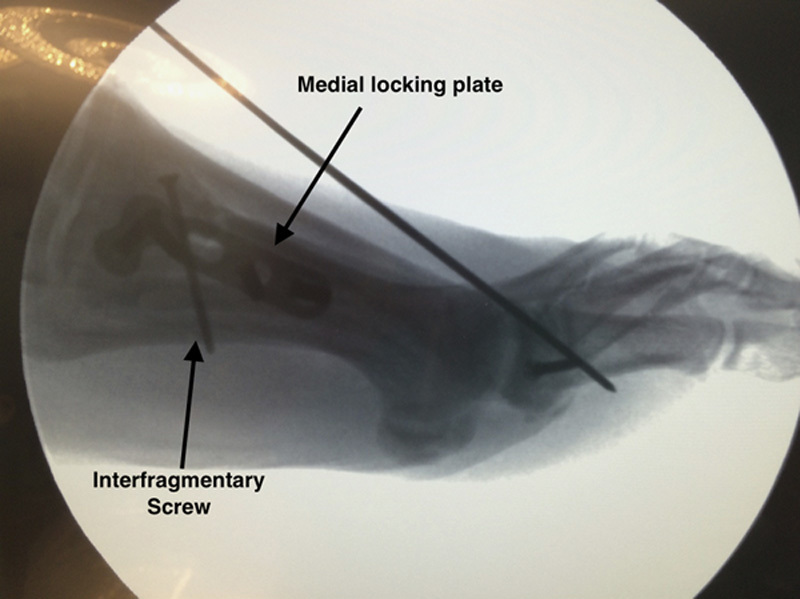
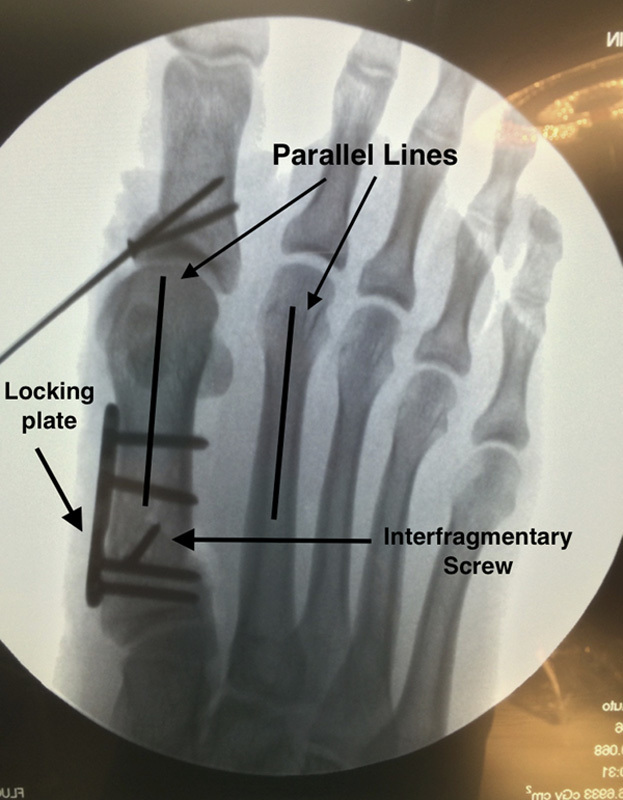
More than 200 different surgical techniques exist for hallux valgus (HV). Some of them are designed for mild, moderate, or severe deformities depending on their correction power. Nevertheless, they all correct only the coronal and/or sagittal plane deformity. Just a handful of them correct the known axial malrotation that exists in most HV cases. This malrotation is one possible factor that could be the source of recurrence of an operated HV as it has been described. We describe a new technique which simultaneously corrects the metatarsal internal rotation and varus deformity by rotating the metatarsal through an oblique plane osteotomy. This is performed with no bone wedge resection. Also, there is a broader bone surface contact than on a transverse proximal osteotomy. This technique is easy to remember and relatively simple to perform in primary and revision cases. The authors results show that it is as safe and effective as other procedures, with some advantages to be discussed.
Levels of evidence: Diagnostic Level 5. See Instructions for Authors for a complete description of levels of evidence.
Keywords: hallux valgus; osteotomy; rotational correction; surgical technique.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Trnka HJ. Osteotomies for hallux valgus correction. Foot Ankle Clin. 2005;10:15–33. - PubMed
-
- Okuda R, Kinoshita M, Yasuda T, et al. Hallux valgus angle as a predictor of recurrence following proximal metatarsal osteotomy. J Orthop Sci. 2011;16:760–764. - PubMed
-
- Okuda R, Kinoshita M, Yasuda T, et al. Postoperative incomplete reduction of the sesamoids as a risk factor for recurrence of hallux valgus. J Bone Joint Surg Am. 2009;91:1637–1645. - PubMed
-
- Wagner E, Ortiz C. Osteotomy considerations in hallux valgus treatment improving the correction power. Foot Ankle Clin N Am. 2012;17:481–498. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials