

A study of dermoscopic features of nail psoriasis
- PMID: 28286468
- PMCID: PMC5340855
- DOI: 10.5114/ada.2017.65618
A study of dermoscopic features of nail psoriasis
Abstract
Introduction: Dermoscopy is a non-invasive imaging method that enables the evaluation of pigmented and non-pigmented skin lesions. More recently, dermoscopy has been recognized as an effective tool in the diagnosis of nail diseases.
Aim: To evaluate the dermoscopic features of nail psoriasis and to assess the relationship between these features and disease severity.
Material and methods: A total of 67 patients with clinically evident nail psoriasis (14 women, 53 men) were prospectively enrolled. Following a thorough clinical examination, patients were graded according to the Nail Psoriasis Severity Index and physician's global assessment score. A dermoscopic examination of all fingernails and toenails was performed using a videodermatoscope. Mann-Whitney U and χ2 tests were used for statistical analysis, with a significance threshold of p < 0.05.
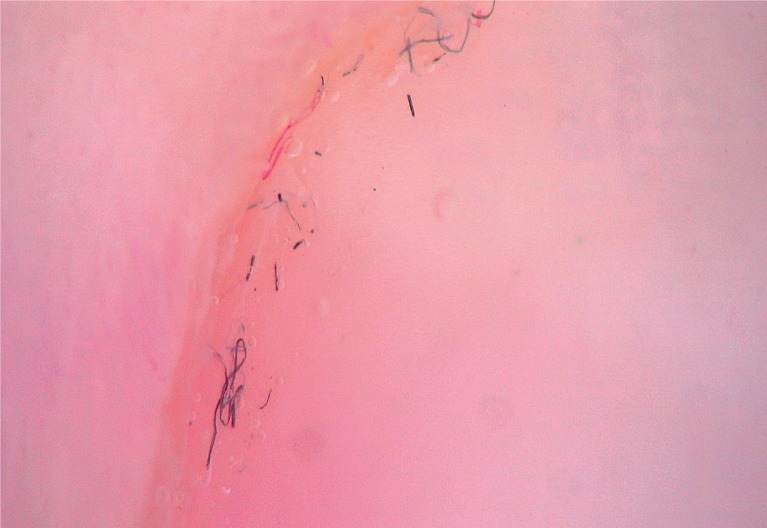
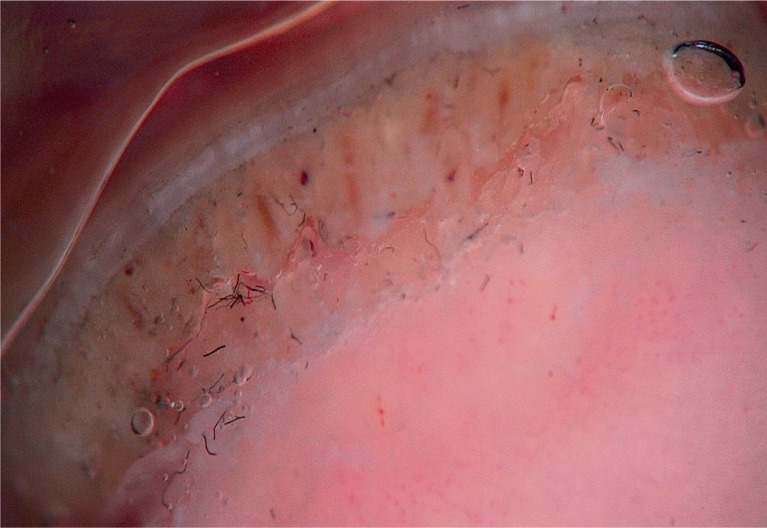
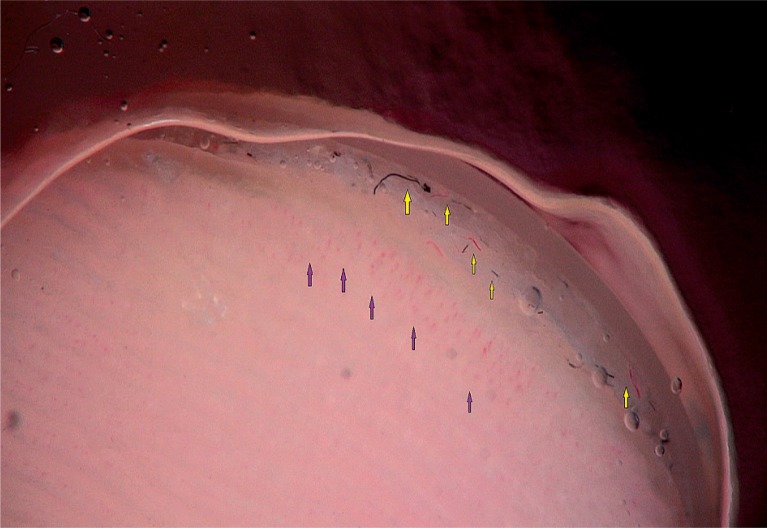
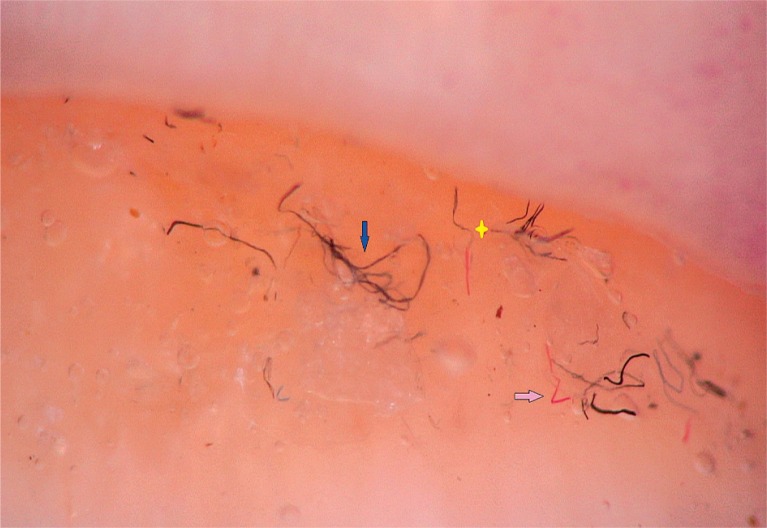
Results: The most frequently observed dermoscopic features were splinter haemorrhage (73.1%), pitting (58.2%), distal onycholysis (55.2%), dilated hyponychial capillaries (35.8%) and the pseudo-fiber sign (34.3%). The pseudo-fiber sign, dilated hyponychial capillaries, nail plate thickening and crumbling, subungual hyperkeratosis, transverse grooves, trachyonychia, pitting and salmon patches were positively associated with disease severity.
Conclusions: The pseudo-fiber sign described in this study appears to be a novel dermoscopic feature of nail psoriasis. We have demonstrated positive associations between a number of dermoscopic manifestations and disease severity. Further studies are required to support the present findings.
Keywords: dermoscopy; nail; pseudo-fiber sign; psoriasis; severity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures












References
-
- Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370:263–71. - PubMed
-
- Tan ES, Chong WS, Tey HL. Nail psoriasis: a review. Am J Clin Dermatol. 2012;13:375–88. - PubMed
-
- Edwards F, de Berker D. Nail psoriasis: clinical presentation and best practice recommendations. Drugs. 2009;69:2351–61. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical