

Acute appendicitis, inflammatory appendiceal mass and the risk of a hidden malignant tumor: a systematic review of the literature
- PMID: 28286544
- PMCID: PMC5343298
- DOI: 10.1186/s13017-017-0122-9
Acute appendicitis, inflammatory appendiceal mass and the risk of a hidden malignant tumor: a systematic review of the literature
Abstract
Introduction: Acute appendicitis is significantly common. Despite the increased use of computed tomography, the number of perforated cases has been stable in the past three decades. Between 2% and 6% of patients with acute appendicitis present appendiceal mass, often described as inflammatory phlegmon or abscess. Malignant tumors are confirmed by pathological analysis in 0.9-1.4% of all appendectomies performed to treat acute appendicitis. However, recent series demonstrate an elevated incidence of malignancies, ranging from 5.9 to 12%, in patients with inflammatory appendiceal mass.
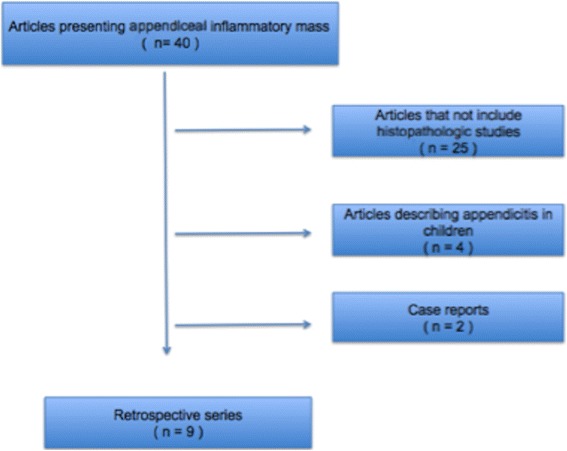
Methods: The analysis was based on a systematic review of the literature. The articles were searched in PubMed for the period from 1987 to 2016. Articles presenting the incidence of the hidden malignancy among patients with appendiceal inflammatory mass were selected. Variables as age, interval appendectomy rate, the incidence of neoplasm, time to surgery, minimally invasive assessment, histology, right colectomy rate and morbidity were analyzed.
Results: A total of 13.244 patients were described as presenting acute appendicitis. Appendiceal tumor is present in approximately 1% of the appendectomies, while the rate of neoplasm varies from 10 to 29% in patients presenting appendiceal inflammatory mass. Interval appendectomies, despite been the minority of the procedures, disregard the higher morbidity associated with right sided colectomies. The review of literature also describes oncologic, histologic and clinical aspects of patients presenting appendiceal neoplasm, describing the most frequent histologic subtypes of this illness.
Conclusion: Hidden appendiceal neoplasm in acute appendicitis are rare, fortunately. However, its incidence is much higher in patients presenting appendiceal inflammatory mass. Hence, interval appendectomy should be considered in this subgroup of patients.
Keywords: Acute appendicits; Appendiceal inflammatory mass; Appendiceal neoplasms; Appendiceal neuroendocrine tumors; Interval appendectomy; Pseudomixoma peritonei.
Figures


References
-
- McBurney C. Experience with early operative interference in cases of disease of the vermiform appendix. N Y Med J. 1889;50:676–84.
-
- De Frances CJ, Cullen KA, Kozak LJ. National Hospital Discharge Survey: 2005 annual summary with detailed diagnosis and procedure data. Vital Health Stat. 2007;1:209. - PubMed
-
- Collins DC. 71,000 human appendix specimens. A final report, summarizing forty years of study. Am J Proctol. 1963;14:265–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
