

Closed reduction with or without adductor tenotomy for developmental dysplasia of the hip presenting at walking age
- PMID: 28286603
- PMCID: PMC5325246
- DOI: 10.1097/BCO.0000000000000478
Closed reduction with or without adductor tenotomy for developmental dysplasia of the hip presenting at walking age
Abstract
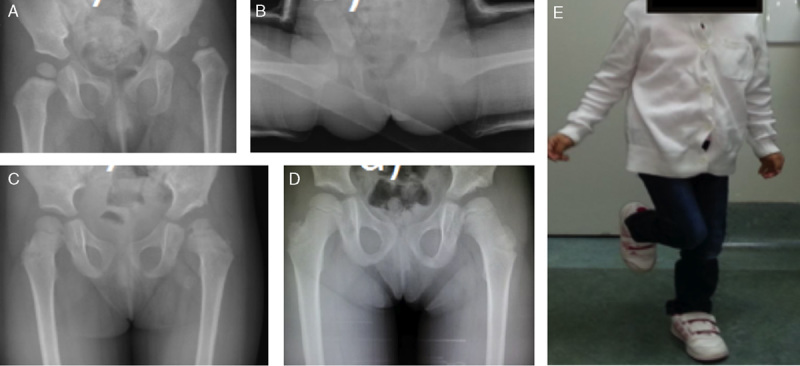
Background: Many children with developmental dislocation of the hip especially in underdeveloped countries reach walking age and still remain undiagnosed, which can be detrimental to their growth and development. Because of the lack medical services often encountered in these regions, it would be attractive to find a cheap and effective treatment. Our work evaluated the results of treatment of these children by closed reduction with or without adductor tenotomy in a prospective study.
Methods: We included 20 patients in this study with 29 affected hips (15 right and 14 left). Nine patients (45%) had bilateral DDH and 11 (55%) had unilateral DDH. There were 18 girls (90%) and two boys (10%) who were followed up for a mean of 21 mo (18-24 mo). Ages ranged from 9 to 36 mo (mean age 18.3 mo). Patients were divided according to age into two groups: between 9-18 mo and from 19-36 mo. The first group included nine patients (14 hips) while the second had 11 patients (15 hips).
Results: In the first group, closed reduction failed in two patients (two hips) during the follow-up period (14.3%) and this necessitated shift to open reduction, while in the second group only one patient (bilateral DDH) had a similar failure (13.3%). We identified four hips with avascular necrosis. Three of them required no further treatment, the remaining hip was openly reduced.
Conclusions: Closed reduction in older children offers a valid and reproducible treatment modality in the hands of an experienced pediatric orthopaedic surgeon as long as there is close follow-up and thorough knowledge of possible complications and their management including the ability to shift timely to open reduction.
Keywords: DDH; abductor brace; closed reduction; conservative treatment; delayed diagnosis; walking age.
Conflict of interest statement
Financial Disclosure: The authors report no conflicts of interest.
Figures
References
-
- Guille JT, Pizzutillo PD, MacEwen GD. Development dysplasia of the hip from birth to six months. J Am Acad Orthop Surg. 2000; 8:232–242. - PubMed
-
- Wirth T, Stratmann L, Hinrichs F. Evolution of late presenting developmental dysplasia of the hip and associated surgical procedures after 14 years of neonatal ultrasound screening. J Bone Joint Surg Br. 2004; 86B:585–589. - PubMed
-
- Schwend RM, Shaw BA, Segal LS. Evaluation and treatment of developmental hip dysplasia in the newborn and infant. Pediatr Clin North Am. 2014; 61:1095–1107. - PubMed
-
- Mulpuri K, Song KM, Goldberg MJ, et al. Detection and nonoperative management of pediatric developmental dysplasia of the hip in infants up to six months of age. J Am Acad Orthop Surg. 2015; 23:202–2055. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials