

Semiautomated Workflow for Clinically Streamlined Glioma Parametric Response Mapping
- PMID: 28286871
- PMCID: PMC5345939
- DOI: 10.18383/j.tom.2016.00181
Semiautomated Workflow for Clinically Streamlined Glioma Parametric Response Mapping
Abstract
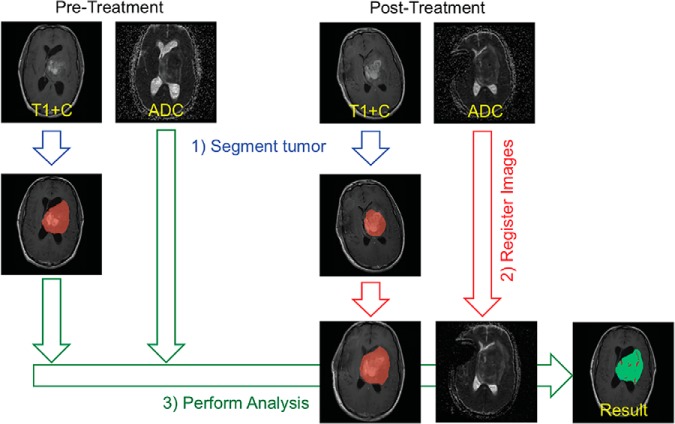
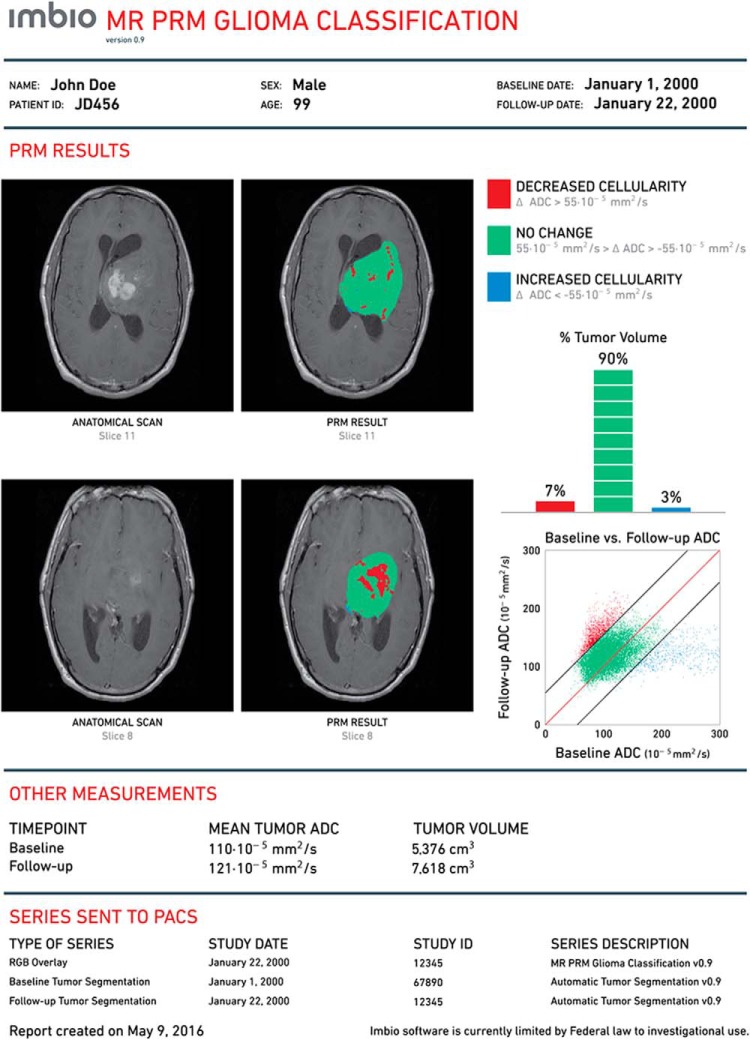
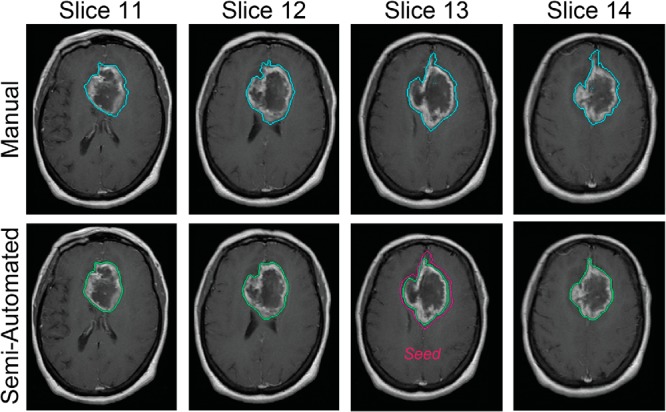
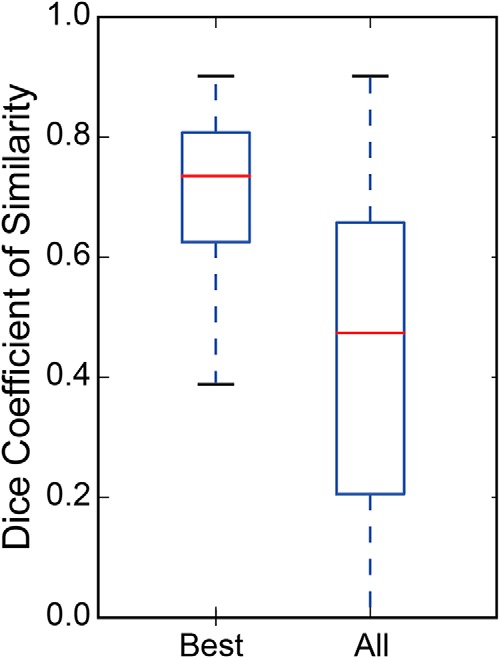
Management of glioblastoma multiforme remains a challenging problem despite recent advances in targeted therapies. Timely assessment of therapeutic agents is hindered by the lack of standard quantitative imaging protocols for determining targeted response. Clinical response assessment for brain tumors is determined by volumetric changes assessed at 10 weeks post-treatment initiation. Further, current clinical criteria fail to use advanced quantitative imaging approaches, such as diffusion and perfusion magnetic resonance imaging. Development of the parametric response mapping (PRM) applied to diffusion-weighted magnetic resonance imaging has provided a sensitive and early biomarker of successful cytotoxic therapy in brain tumors while maintaining a spatial context within the tumor. Although PRM provides an earlier readout than volumetry and sometimes greater sensitivity compared with traditional whole-tumor diffusion statistics, it is not routinely used for patient management; an automated and standardized software for performing the analysis and for the generation of a clinical report document is required for this. We present a semiautomated and seamless workflow for image coregistration, segmentation, and PRM classification of glioblastoma multiforme diffusion-weighted magnetic resonance imaging scans. The software solution can be integrated using local hardware or performed remotely in the cloud while providing connectivity to existing picture archive and communication systems. This is an important step toward implementing PRM analysis of solid tumors in routine clinical practice.
Keywords: diffusion; glioma; parametric response mapping.
Conflict of interest statement
Conflict of Interest: BDR has financial interest in Imbio, LLC. BDR and TLC are eligible to receive royalties using this technology.
Figures
Similar articles
-
A generalized parametric response mapping method for analysis of multi-parametric imaging: A feasibility study with application to glioblastoma.Med Phys. 2017 Nov;44(11):6074-6084. doi: 10.1002/mp.12562. Epub 2017 Oct 13. Med Phys. 2017. PMID: 28875538
-
Comparison of unsupervised classification methods for brain tumor segmentation using multi-parametric MRI.Neuroimage Clin. 2016 Sep 30;12:753-764. doi: 10.1016/j.nicl.2016.09.021. eCollection 2016. Neuroimage Clin. 2016. PMID: 27812502 Free PMC article.
-
Automated and Semiautomated Segmentation of Rectal Tumor Volumes on Diffusion-Weighted MRI: Can It Replace Manual Volumetry?Int J Radiat Oncol Biol Phys. 2016 Mar 15;94(4):824-31. doi: 10.1016/j.ijrobp.2015.12.017. Epub 2015 Dec 17. Int J Radiat Oncol Biol Phys. 2016. PMID: 26972655
-
Diffusion-weighted MR of the brain: methodology and clinical application.Radiol Med. 2005 Mar;109(3):155-97. Radiol Med. 2005. PMID: 15775887 Review. English, Italian.
-
Relevance of magnetic resonance imaging for early detection and diagnosis of Alzheimer disease.Med Clin North Am. 2013 May;97(3):399-424. doi: 10.1016/j.mcna.2012.12.013. Epub 2013 Feb 1. Med Clin North Am. 2013. PMID: 23642578 Review.
Cited by
-
Parametric Response Mapping of FLAIR MRI Provides an Early Indication of Progression Risk in Glioblastoma.Acad Radiol. 2021 Dec;28(12):1711-1720. doi: 10.1016/j.acra.2020.08.015. Epub 2020 Sep 11. Acad Radiol. 2021. PMID: 32928633 Free PMC article.
-
Local aortic aneurysm wall expansion measured with automated image analysis.JVS Vasc Sci. 2021 Dec 8;3:48-63. doi: 10.1016/j.jvssci.2021.11.004. eCollection 2022. JVS Vasc Sci. 2021. PMID: 35146458 Free PMC article.
-
Vascular Deformation Mapping (VDM) of Thoracic Aortic Enlargement in Aneurysmal Disease and Dissection.Tomography. 2017 Sep;3(3):163-173. doi: 10.18383/j.tom.2017.00015. Tomography. 2017. PMID: 29124128 Free PMC article.
References
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, Hau P, Brandes AA, Gijtenbeek J, Marosi C, Vecht CJ, Mokhtari K, Wesseling P, Villa S, Eisenhauer E, Gorlia T, Weller M, Lacombe D, Cairncross JG, Mirimanoff RO, European Organisation for R, Treatment of Cancer Brain T, Radiation Oncology G, National Cancer Institute of Canada Clinical Trials Group. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10(5):459–466. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, Gorlia T, Allgeier A, Lacombe D, Cairncross JG, Eisenhauer E, Mirimanoff RO, European Organisation for R, Treatment of Cancer Brain T, Radiotherapy G, National Cancer Institute of Canada Clinical Trials Group. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Macdonald DR, Cascino TL, Schold SC Jr., Cairncross JG. Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol. 1990;8(7):1277–1280. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources