

The molecular biology of pelvi-ureteric junction obstruction
- PMID: 28286898
- PMCID: PMC5859056
- DOI: 10.1007/s00467-017-3629-0
The molecular biology of pelvi-ureteric junction obstruction
Abstract
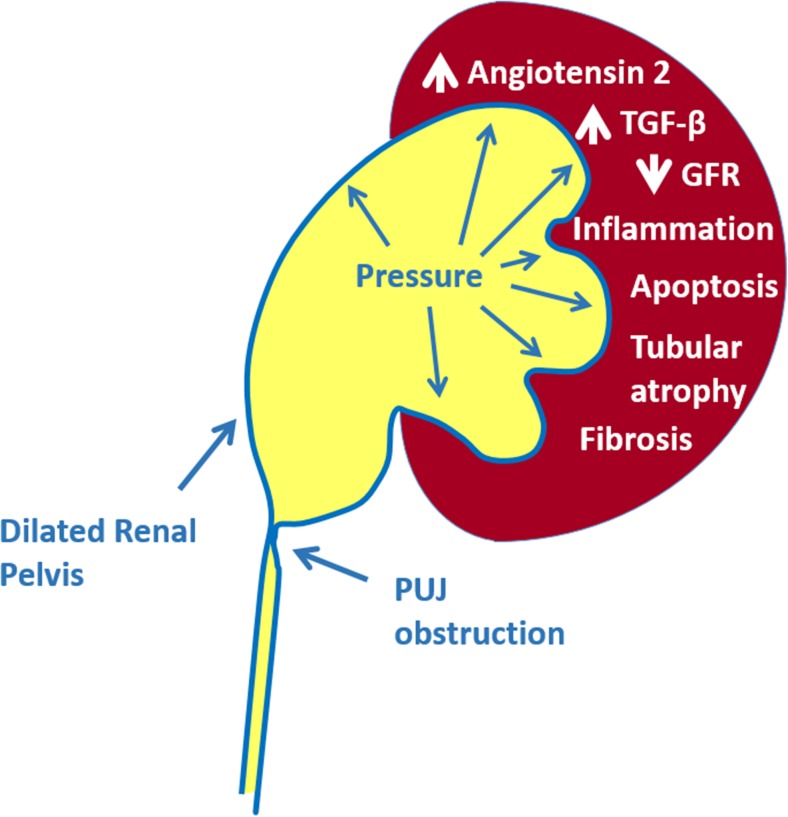
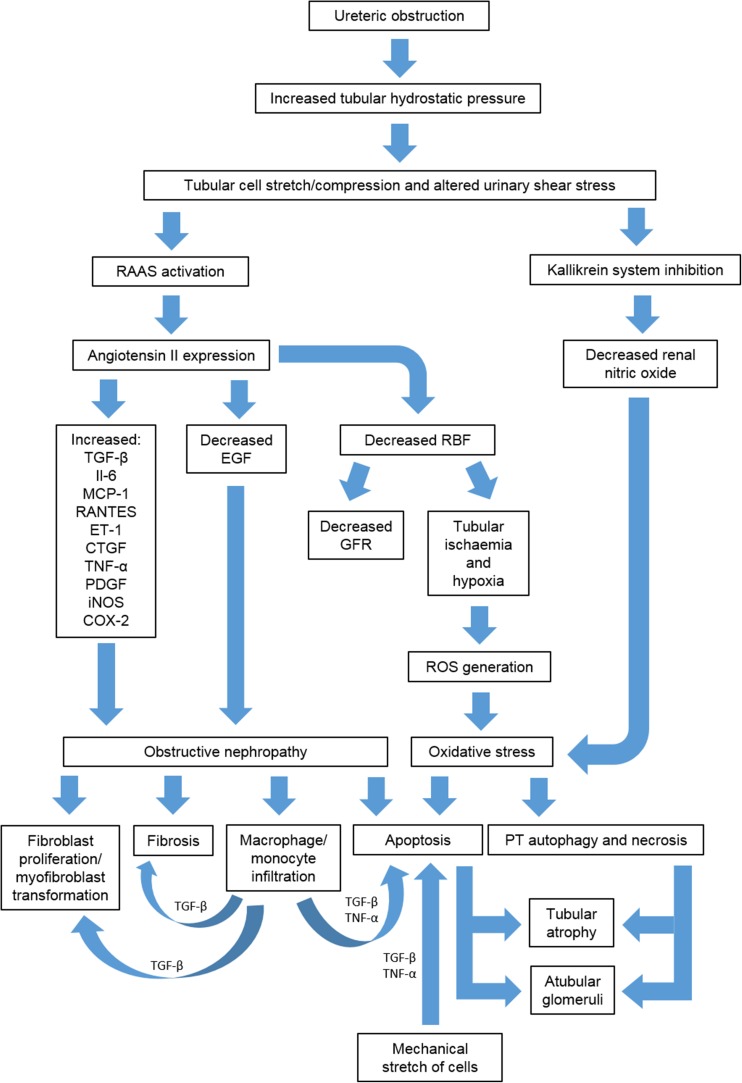
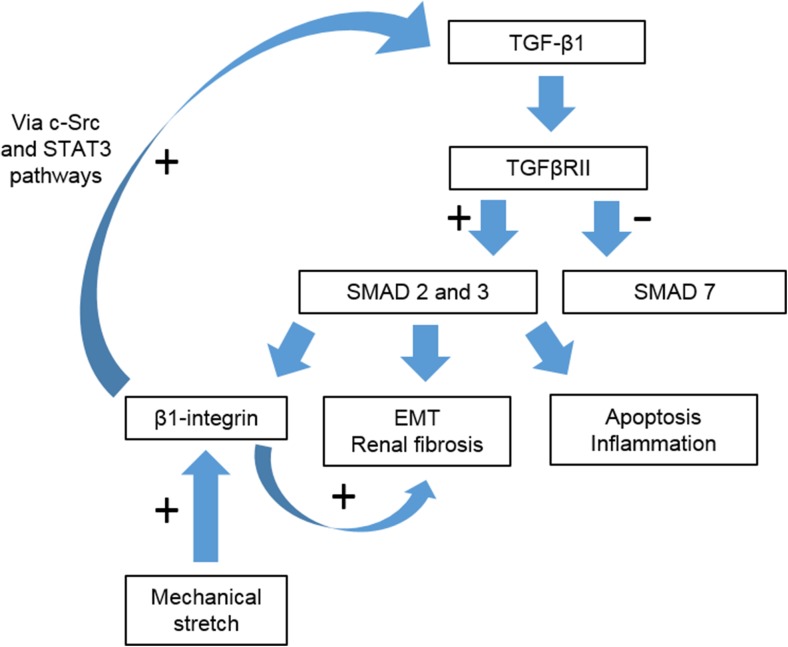
Over recent years routine ultrasound scanning has identified increasing numbers of neonates as having hydronephrosis and pelvi-ureteric junction obstruction (PUJO). This patient group presents a diagnostic and management challenge for paediatric nephrologists and urologists. In this review we consider the known molecular mechanisms underpinning PUJO and review the potential of utilising this information to develop novel therapeutics and diagnostic biomarkers to improve the care of children with this disorder.
Keywords: Aetiology; Biomarker; Hydronephrosis; Molecular biology; Pelvi-ureteric junction obstruction.
Conflict of interest statement
Funding
Laura Jackson is funded by a joint Royal College of Surgeons of England/British Association of Paediatric Surgeons Fellowship (Awarded 2014). Richard Coward is funded by the Medical Research Council as a Senior Clinical Fellow MR/K010492/1.
Conflict of interest
The authors declare that they have no conflict of interest.
Figures
References
-
- Brussels Free University Perinatal Nephrology Study Group. Ismaili K, Avni FE, Wissing KM, Hall M. Long-term clinical outcome of infants with mild and moderate fetal pyelectasis: validation of neonatal ultrasound as a screening tool to detect significant nephrouropathies. J Pediatr. 2004;144:759–765. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
