

Usefulness of the Waist Circumference-to-Height Ratio in Screening for Obesity and Metabolic Syndrome among Korean Children and Adolescents: Korea National Health and Nutrition Examination Survey, 2010-2014
- PMID: 28287410
- PMCID: PMC5372919
- DOI: 10.3390/nu9030256
Usefulness of the Waist Circumference-to-Height Ratio in Screening for Obesity and Metabolic Syndrome among Korean Children and Adolescents: Korea National Health and Nutrition Examination Survey, 2010-2014
Abstract
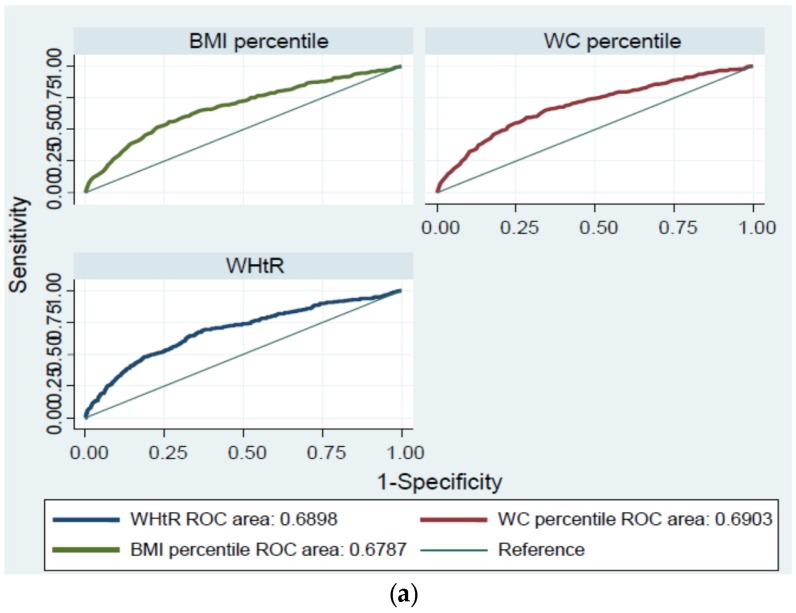
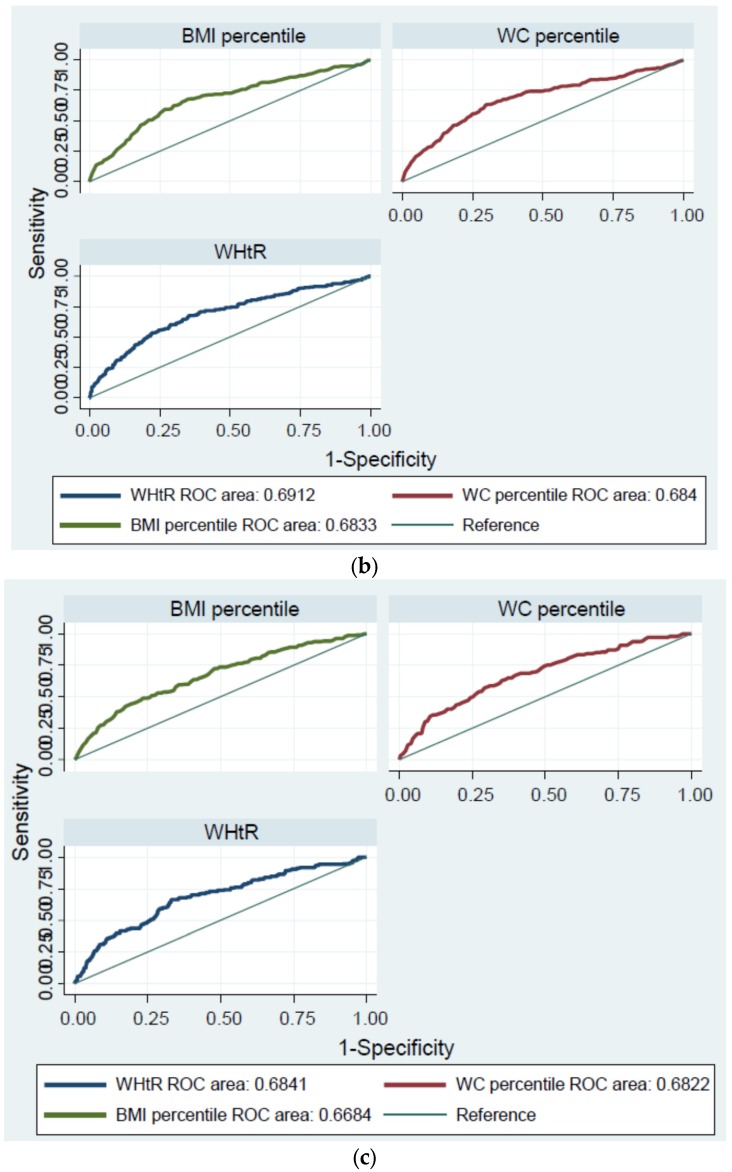
The aims of this study were to assess the diagnostic value of the weight-to-height ratio (WHtR) for the detection of obesity and metabolic syndrome (MS) in Korean children and adolescents, and to determine the advantages of WHtR as a population-based screening tool in comparison with other obesity indicators, such as body mass index (BMI) and waist circumference (WC). We performed a cross-sectional analysis of data from 3057 children and adolescents (1625 boys, 1332 girls) aged 10-19 years who were included in the fifth Korean National Health and Nutrition Examination Survey (KNHANES, 2010-2012) up to the second year of the sixth KNHANES (2013-2014). Receiver operation characteristic (ROC) curves were generated to determine the optimal cutoff value and accuracy of WHtR for predicting individual obesity indicators or more than two non-WC components of MS. The area under the ROC curve (AUC) is a measure of the diagnostic power of a test. A perfect test will have an AUC of 1.0, and an AUC equal to 0.5 means that the test performs no better than chance. The optimal WHtR cutoff for the evaluation of general obesity and central obesity was 0.50 in boys and 0.47-0.48 in girls, and the AUC was 0.9. Regarding the assessment of each MS risk factor, the optimal WHtR cutoff was 0.43-0.50 in boys and 0.43-0.49 in girls, and these cutoffs were statistically significant only for the detection of high triglyceride and low High-density lipoprotein (HDL) cholesterol levels. When a pairwise comparison of the AUCs was conducted between WHtR and BMI/WC percentiles to quantify the differences in power for MS screening, the WHtR AUC values (boys, 0.691; girls, 0.684) were higher than those of other indices; however, these differences were not statistically significant (boys, p = 0.467; girls, p = 0.51). The WHtR cutoff value was 0.44 (sensitivity, 67.7%; specificity, 64.6%) for boys and 0.43 (sensitivity, 66.4%; specificity, 66.9%) for girls. There was no significant difference between the diagnostic power of WHtR and that of BMI/WC when screening for MS. Although the use of WHtR was not superior, WHtR is still useful as a screening tool for metabolic problems related to obesity because of its convenience.
Keywords: adolescents; body mass index; children; cutoff values; metabolic syndrome; obesity; overweight; waist circumference; waist-to-height ratio.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Murray C.J., Vos T., Lozano R., Naghavi M., Flaxman A.D., Michaud C., Ezzati M., Shibuya K., Salomon J.A., Abdalla S. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet. 2013;380:2197–2223. doi: 10.1016/S0140-6736(12)61689-4. - DOI - PubMed
-
- Korea Centers for Disease Control and Prevention . Korea Health Statistics 2014: Korea National Health and Nutrition Examination Survey (KNHANES VI-2) Ministry of Health and Welfare; Seoul, Korea: 2014.
-
- Cho S.J., Kim E.Y., Rho Y.I., Yang E.S., Park Y.B., Moon K.R., Lee C.G. The long-term follow-up studies of childhood obesity after puberty. Korean J. Pediatr. Gastroenterol. Nutr. 2003;6:47–53.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
