

Soft-Tissue Sarcomas of the Abdomen and Pelvis: Radiologic-Pathologic Features, Part 1-Common Sarcomas: From the Radiologic Pathology Archives
- PMID: 28287938
- PMCID: PMC5416744
- DOI: 10.1148/rg.2017160157
Soft-Tissue Sarcomas of the Abdomen and Pelvis: Radiologic-Pathologic Features, Part 1-Common Sarcomas: From the Radiologic Pathology Archives
Abstract
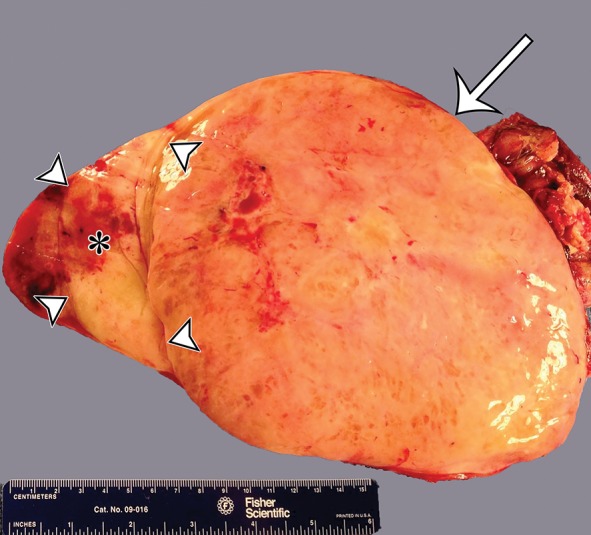
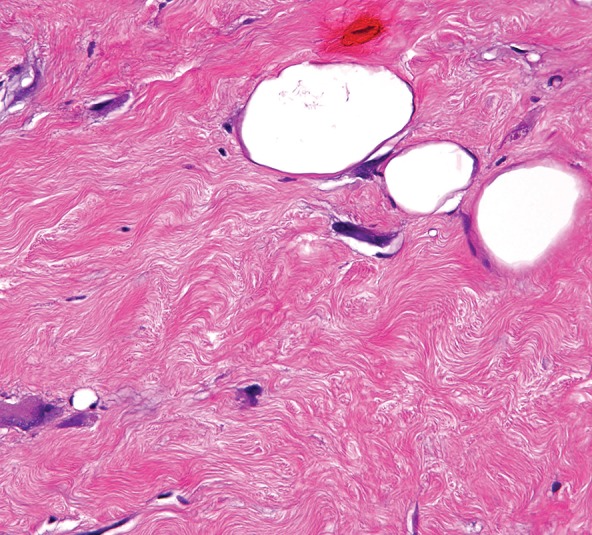
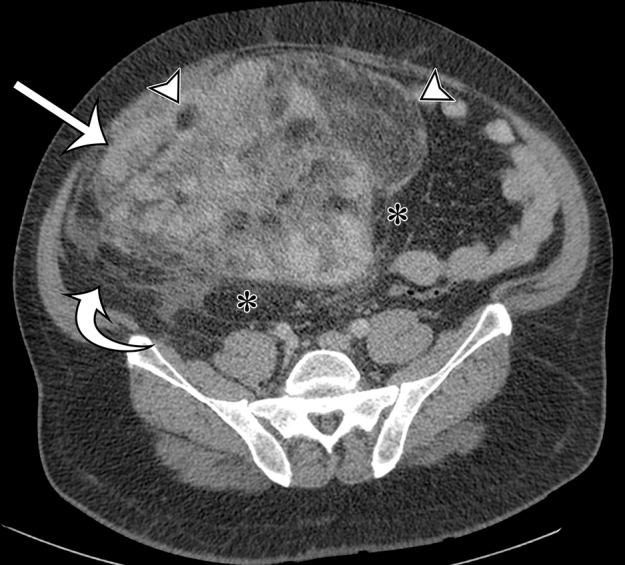
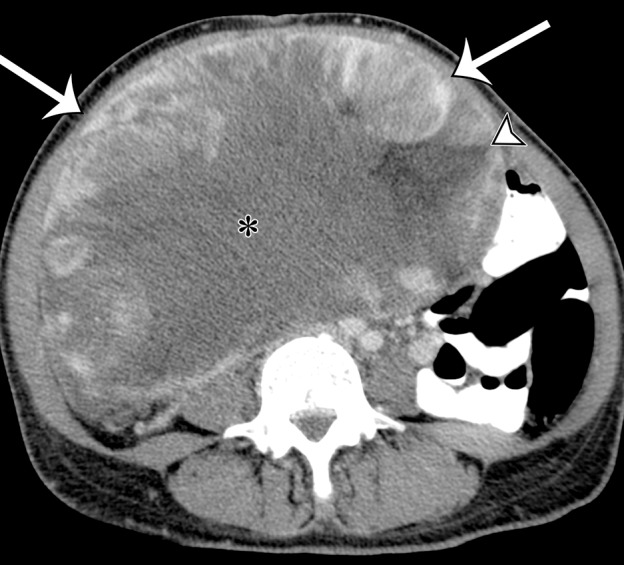
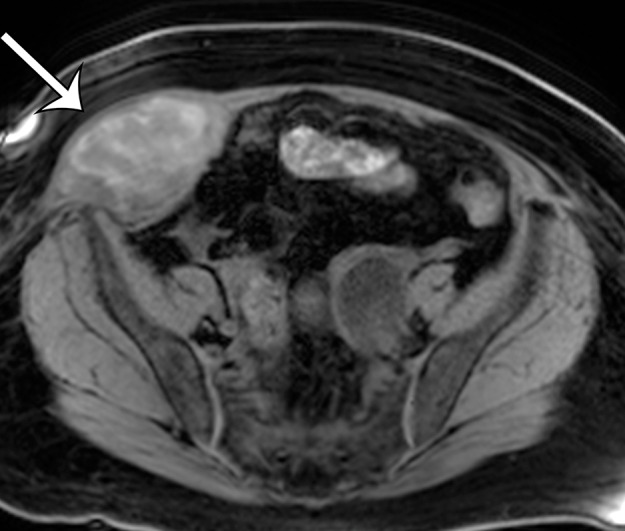
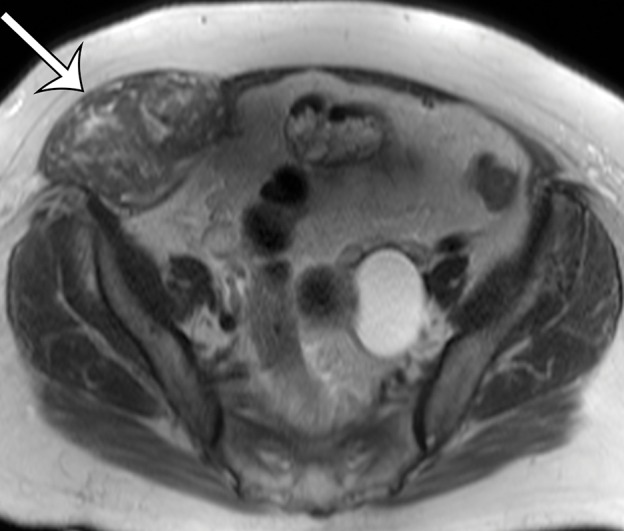
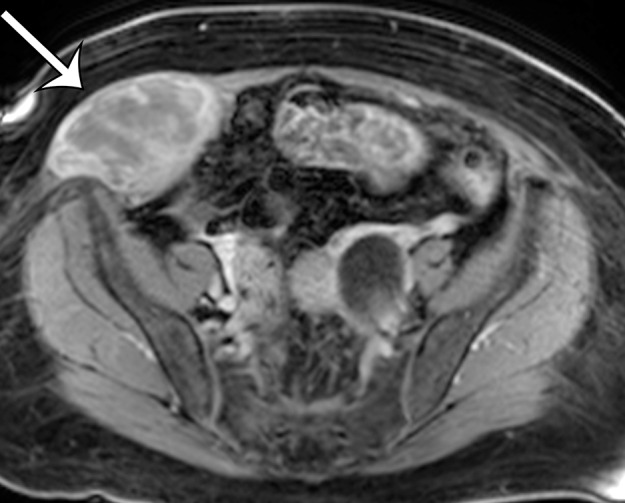
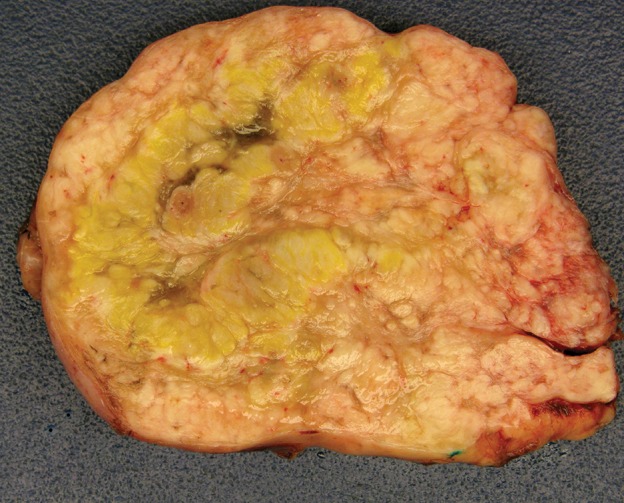
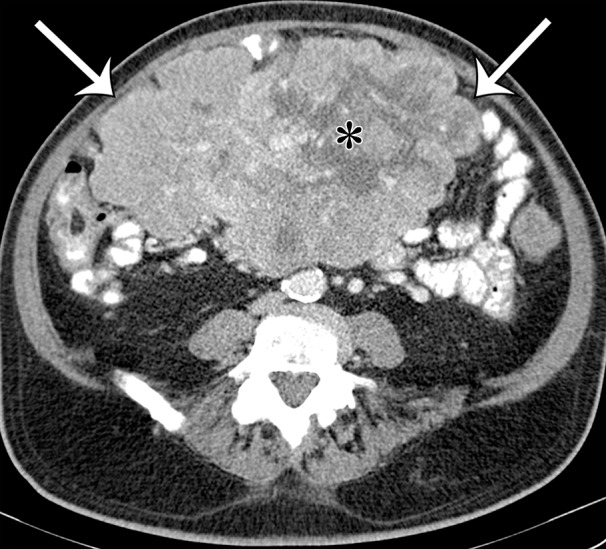
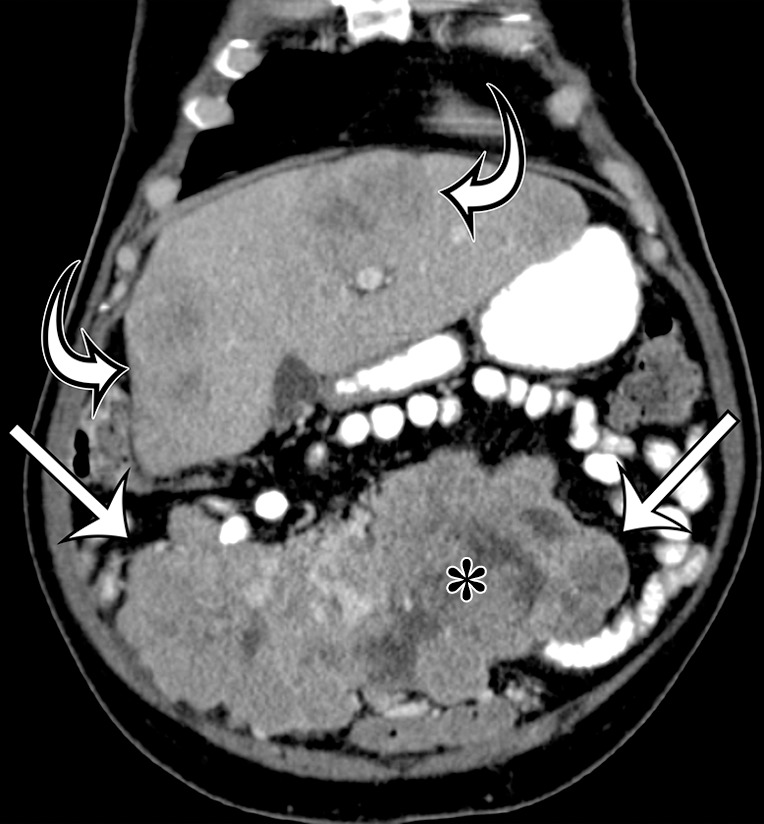
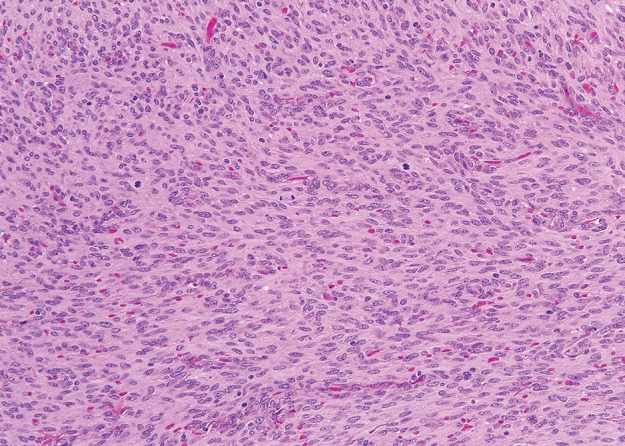
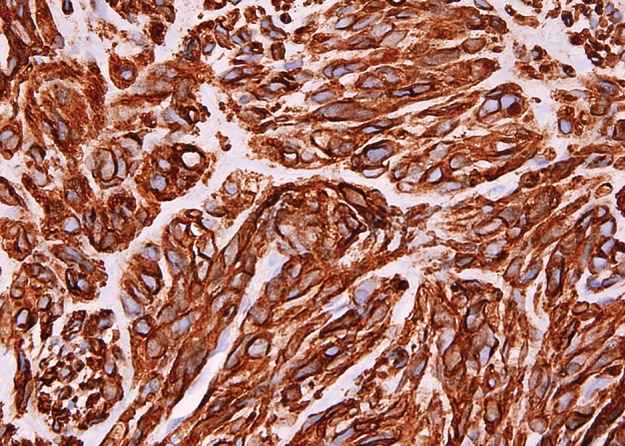
Soft-tissue sarcomas are a diverse group of rare mesenchymal malignancies that can arise at any location in the body and affect all age groups. These sarcomas are most common in the extremities, trunk wall, retroperitoneum, and head and neck. In the adult population, soft-tissue sarcomas arising in the abdomen and pelvis are often large masses at the time of diagnosis because they are usually clinically silent or cause vague or mild symptoms until they invade or compress vital organs. In contrast, soft-tissue sarcomas arising from the abdominal wall come to clinical attention earlier in the course of disease because they cause a palpable mass, abdominal wall deformity, or pain that is more clinically apparent. The imaging features of abdominal and pelvic sarcomas and abdominal wall sarcomas can be nonspecific and overlap with more common pathologic conditions, making diagnosis difficult or, in some cases, delaying diagnosis. Liposarcoma (well-differentiated and dedifferentiated liposarcomas), leiomyosarcoma, and gastrointestinal stromal tumor (GIST) are the most common intra-abdominal primary sarcomas. Any soft-tissue sarcoma can arise in the abdominal wall. Knowledge of the classification and pathologic features of soft-tissue sarcomas, the anatomic locations where they occur, and their cross-sectional imaging features helps the radiologist establish the diagnosis or differential diagnosis so that patients with soft-tissue sarcomas can receive optimal treatment and management. In part 1 of this article, the most common soft-tissue sarcomas (liposarcoma, leiomyosarcoma, and GIST) are reviewed, with a discussion on anatomic locations, classification, clinical considerations, and differential diagnosis. Part 2 will focus on the remainder of the soft-tissue sarcomas occurring in the abdomen and pelvis.
Figures








References
-
- Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F, eds. WHO classification of tumours of soft tissue and bone. 4th ed. Lyon, France: IARC, 2013; 10–11.
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016;66(1):7–30. - PubMed
-
- Cormier JN, Pollock RE. Soft tissue sarcomas. CA Cancer J Clin 2004;54(2):94–109. - PubMed
-
- Baheti AD, O’Malley RB, Kim S, et al. Soft-tissue sarcomas: an update for radiologists based on the revised 2013 World Health Organization classification. AJR Am J Roentgenol 2016;206(5):924–932. - PubMed
-
- Gerota D. Beitrage zur kenntnis des befestigungsapparates der niere. Arch Anat Entwicklungsgesch 1895;19:265–286.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
