

Association of Intensive Blood Pressure Control and Kidney Disease Progression in Nondiabetic Patients With Chronic Kidney Disease: A Systematic Review and Meta-analysis
- PMID: 28288249
- PMCID: PMC5818822
- DOI: 10.1001/jamainternmed.2017.0197
Association of Intensive Blood Pressure Control and Kidney Disease Progression in Nondiabetic Patients With Chronic Kidney Disease: A Systematic Review and Meta-analysis
Erratum in
-
Omission of Data and Errors in Meta-analysis.JAMA Intern Med. 2017 Nov 1;177(11):1703. doi: 10.1001/jamainternmed.2017.5375. JAMA Intern Med. 2017. PMID: 28975205 Free PMC article. No abstract available.
Abstract
Importance: The optimal blood pressure (BP) target remains debated in nondiabetic patients with chronic kidney disease (CKD).
Objective: To compare intensive BP control (<130/80 mm Hg) with standard BP control (<140/90 mm Hg) on major renal outcomes in patients with CKD without diabetes.
Data sources: Searches of PubMed, MEDLINE, Embase, and Cochrane Library for publications up to March 24, 2016.
Study selection: Randomized clinical trials that compared an intensive vs a standard BP target in nondiabetic adults with CKD, reporting changes in glomerular filtration rate (GFR), doubling of serum creatinine level, 50% reduction in GFR, end-stage renal disease (ESRD), or all-cause mortality.
Data extraction and synthesis: Random-effects meta-analyses for pooling effect measures. Meta-regression and subgroup analyses for exploring heterogeneity.
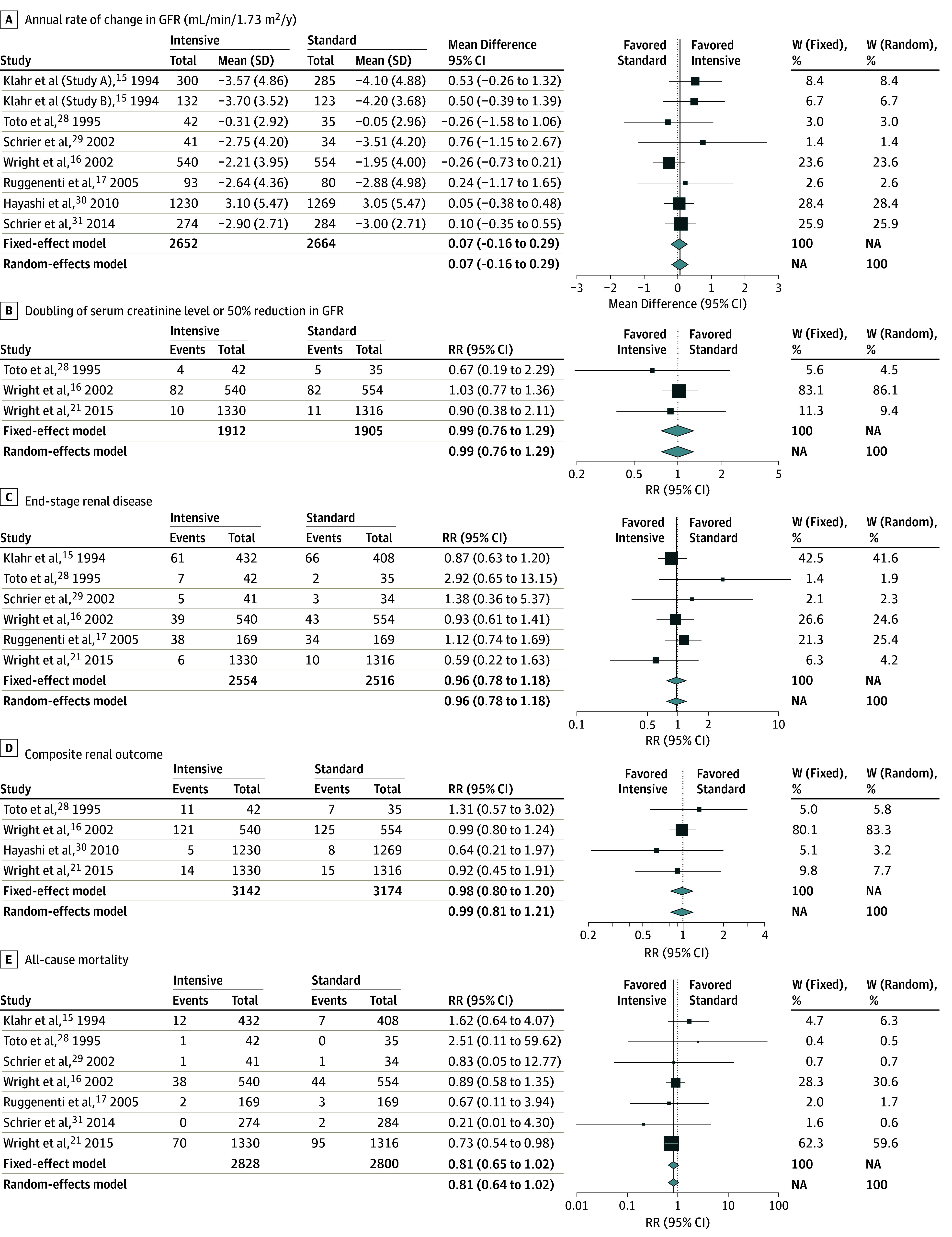
Main outcomes and measures: Differences in annual rate of change in GFR were expressed as mean differences with 95% CIs. Differences in doubling of serum creatinine or 50% reduction in GFR, ESRD, composite renal outcome, and all-cause mortality were expressed as risk ratios (RRs) with 95% CIs.
Results: We identified 9 trials with 8127 patients and a median follow-up of 3.3 years. Compared with standard BP control, intensive BP control did not show a significant difference on the annual rate of change in GFR (mean difference, 0.07; 95% CI, -0.16 to 0.29 mL/min/1.73 m2/y), doubling of serum creatinine level or 50% reduction in GFR (RR, 0.99; 95% CI, 0.76-1.29), ESRD (RR, 0.96; 95% CI, 0.78-1.18), composite renal outcome (RR, 0.99; 95% CI, 0.81-1.21), or all-cause mortality (RR, 0.95; 95% CI, 0.66-1.37). Nonblacks and patients with higher levels of proteinuria showed a trend of lower risk of kidney disease progression with intensive BP control.
Conclusions and relevance: Targeting BP below the current standard did not provide additional benefit for renal outcomes compared with standard treatment during a follow-up of 3.3 years in patients with CKD without diabetes. However, nonblack patients or those with higher levels of proteinuria might benefit from the intensive BP-lowering treatments.
Conflict of interest statement
Figures
Comment in
-
Omission of Data and Errors in Meta-analysis.JAMA Intern Med. 2017 Nov 1;177(11):1694-1695. doi: 10.1001/jamainternmed.2017.5327. JAMA Intern Med. 2017. PMID: 28975224 No abstract available.
-
Intensive Blood Pressure Control in Autosomal Dominant Polycystic Kidney Disease-How Safe Is It?JAMA Intern Med. 2017 Nov 1;177(11):1694. doi: 10.1001/jamainternmed.2017.4907. JAMA Intern Med. 2017. PMID: 29114789 No abstract available.
-
Intensive Blood Pressure Control in Autosomal Dominant Polycystic Kidney Disease-How Safe Is It?-Reply.JAMA Intern Med. 2017 Nov 1;177(11):1695-1696. doi: 10.1001/jamainternmed.2017.4925. JAMA Intern Med. 2017. PMID: 29114798 No abstract available.
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296-1305. - PubMed
-
- Wu HY, Peng YS, Chiang CK, et al. Diagnostic performance of random urine samples using albumin concentration vs ratio of albumin to creatinine for microalbuminuria screening in patients with diabetes mellitus: a systematic review and meta-analysis. JAMA Intern Med. 2014;174(7):1108-1115. - PubMed
-
- Wen CP, Cheng TY, Tsai MK, et al. All-cause mortality attributable to chronic kidney disease: a prospective cohort study based on 462 293 adults in Taiwan. Lancet. 2008;371(9631):2173-2182. - PubMed
-
- Jha V, Garcia-Garcia G, Iseki K, et al. Chronic kidney disease: global dimension and perspectives. Lancet. 2013;382(9888):260-272. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
