

Population coverage of artemisinin-based combination treatment in children younger than 5 years with fever and Plasmodium falciparum infection in Africa, 2003-2015: a modelling study using data from national surveys
- PMID: 28288746
- PMCID: PMC5450656
- DOI: 10.1016/S2214-109X(17)30076-1
Population coverage of artemisinin-based combination treatment in children younger than 5 years with fever and Plasmodium falciparum infection in Africa, 2003-2015: a modelling study using data from national surveys
Abstract
Background: Artemisinin-based combination therapies (ACTs) are the most effective treatment for uncomplicated Plasmodium falciparum malaria infection. A commonly used indicator for monitoring and assessing progress in coverage of malaria treatment is the proportion of children younger than 5 years with reported fever in the previous 14 days who have received an ACT. We propose an improved indicator that incorporates parasite infection status (as assessed by a rapid diagnostic test [RDT]), which is available in recent household surveys. In this study we estimated the annual proportion of children younger than 5 years with fever and a positive RDT in Africa who received an ACT in 2003-15.
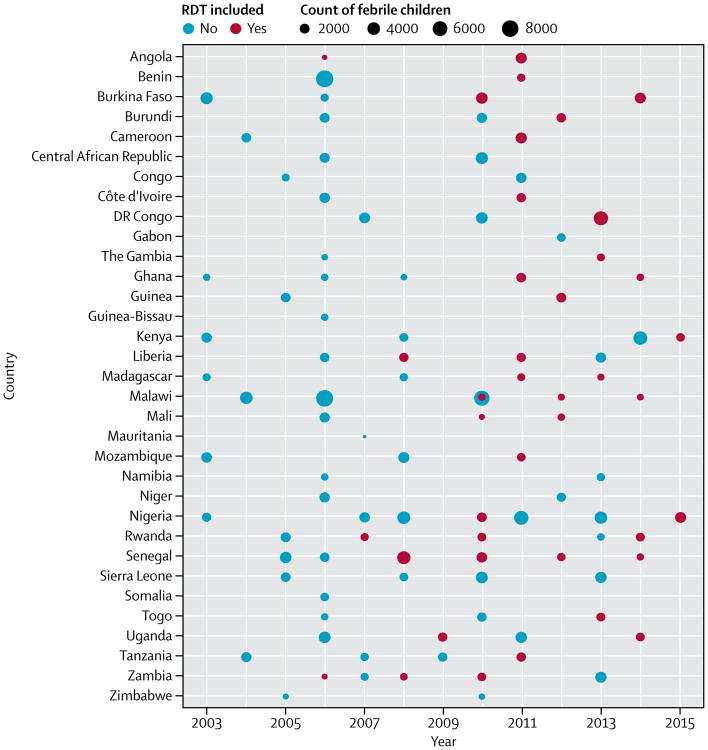
Methods: Our modelling study used cross-sectional data on treatment for fever and RDT status for children younger than 5 years compiled from all nationally available representative household surveys (the Malaria Indicator Surveys, Demographic and Health Surveys, and Multiple Indicator Cluster Surveys) across sub-Saharan Africa between 2003 and 2015. Estimates for the proportion of children younger than 5 years with a fever within the previous 14 days and P falciparum infection assessed by RDT who received an ACT were incorporated in a generalised additive mixed model, including data on ACT distributions, to estimate coverage across all countries and time periods. We did random effects meta-analyses to examine individual, household, and community effects associated with ACT coverage.
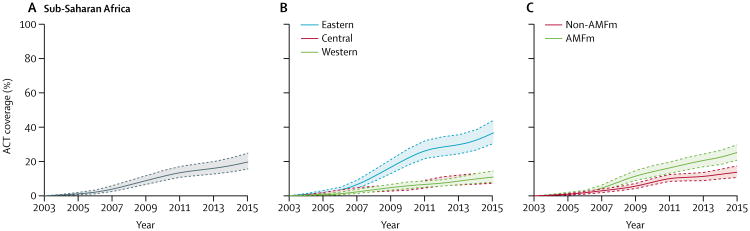
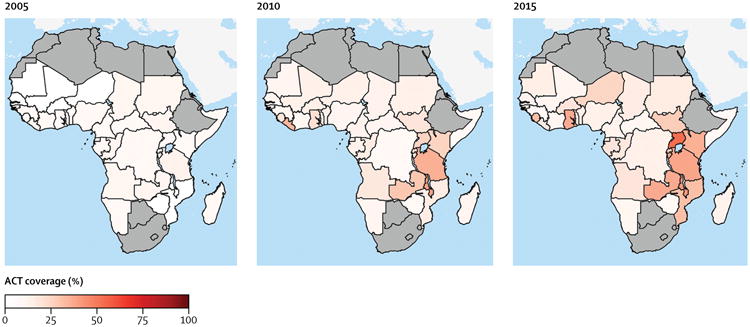
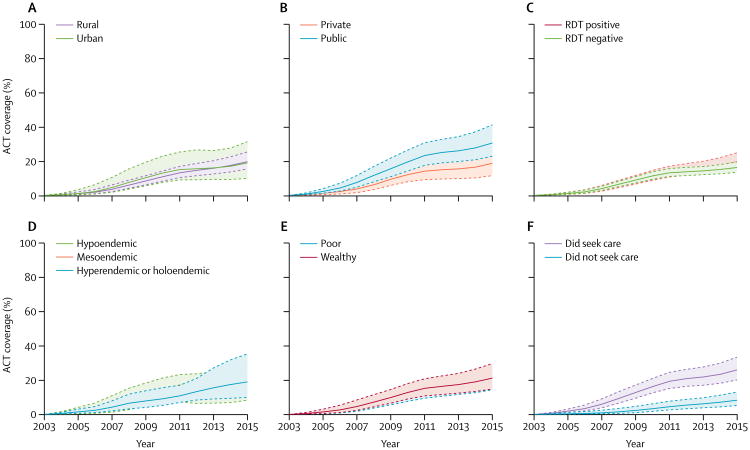
Findings: We obtained data on 201 704 children younger than 5 years from 103 surveys (22 MIS, 61 DHS, and 20 MICS) across 33 countries. RDT results were available for 40 of these surveys including 40 261 (20%) children, and we predicted RDT status for the remaining 161 443 (80%) children. Our results showed that ACT coverage in children younger than 5 years with a fever and P falciparum infection increased across sub-Saharan Africa in 2003-15, but even in 2015, only 19·7% (95% CI 15·6-24·8) of children younger than 5 years with a fever and P falciparum infection received an ACT. In meta-analyses, children younger than 5 years were more likely to receive an ACT for fever and P falciparum infection if they lived in an urban area (vs rural area; odds ratio [OR] 1·18, 95% CI 1·06-1·31), had household wealth above the national median (vs wealth below the median; OR 1·26, 1·16-1·39), had a caregiver with any education (vs no education; OR 1·31, 1·22-1·41), had a household insecticide-treated net (ITN; vs no ITN; OR 1·21, 1·13-1·29), were older than 2 years (vs ≤2 years; OR 1·09, 1·01-1·17), or lived in an area with a higher mean P falciparum prevalence in children aged 2-10 years (OR 1·12, 1·02-1·23). In the subgroup of children for whom treatment was sought, those who sought treatment in the public sector were more likely to receive an ACT (vs the private sector; OR 3·18, 2·67-3·78).
Interpretation: Despite progress during the 2003-15 malaria programme, ACT treatment for children with malaria remains unacceptably low. More work is needed at the country level to understand how health-care access, service delivery, and ACT supply might be improved to ensure appropriate treatment for all children with malaria.
Funding: US President's Malaria Initiative and Medicines for Malaria Venture.
Copyright © 2017 The Authors. Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Improving estimation of ACT treatment coverage in Africa.Lancet Glob Health. 2017 Apr;5(4):e375-e376. doi: 10.1016/S2214-109X(17)30087-6. Lancet Glob Health. 2017. PMID: 28288736 No abstract available.
References
-
- WHO. Geneva: World Health Organization; 2015. [accessed March 1, 2016]. Achieving the malaria MDG target: reversing the incidence of malaria 2000–2015. https://www.unicef.org/publications/fles/Achieving_the_Malaria_MDG_Targe....
-
- International Artemisinin Study Group. Artesunate combinations for treatment of malaria: meta-analysis. Lancet. 2004;363:9–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
