

Molecular Pathways: Oncologic Pathways and Their Role in T-cell Exclusion and Immune Evasion-A New Role for the AXL Receptor Tyrosine Kinase
- PMID: 28289089
- PMCID: PMC5474155
- DOI: 10.1158/1078-0432.CCR-17-0189
Molecular Pathways: Oncologic Pathways and Their Role in T-cell Exclusion and Immune Evasion-A New Role for the AXL Receptor Tyrosine Kinase
Abstract
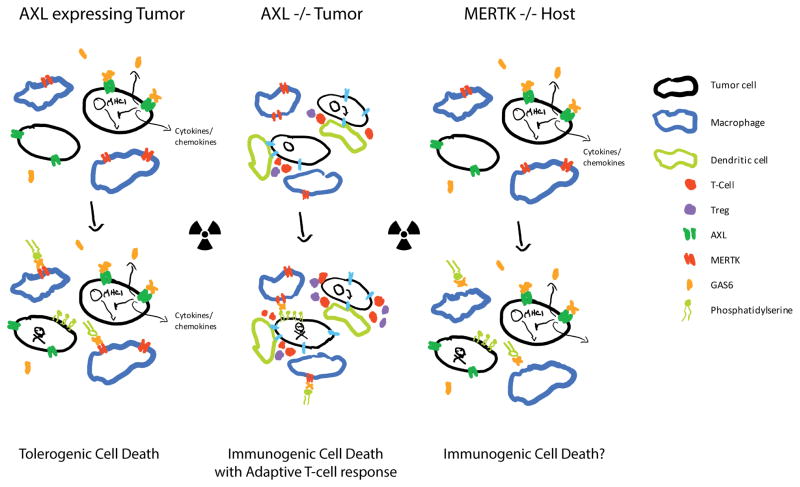
With the clinical impact of CTLA-4 and PD-1/PD-L1 immune checkpoint therapies, widespread interest in cancer immunotherapy has been ignited. However, the rate and extent of clinical responses to approved therapies are limited and often nonexistent in many solid tumors. This is partially because immune checkpoint therapies are most effective against T-cell-inflamed tumors, and non-T-cell-inflamed or T-cell-excluded tumors remain a significant barrier. New strategies are needed to overcome immune resistance mechanisms that arise during tumor development, which result in T-cell exclusion. Approaches may need to be combined with conventional therapies such as chemotherapy, radiotherapy, and molecularly targeted therapy, and many clinical trials are ongoing. This review discusses the challenge of T-cell exclusion and innate oncologic pathways that contribute to this problem, including β-catenin, STAT3, NF-κB, PTEN, and AXL tyrosine kinase. The GAS6/AXL pathway is of interest immunologically, as its targeting can lead to greater antitumor immune responses after radiotherapy. In addition, several targeted therapies that are selective and nonselective for AXL are in preclinical and clinical development in acute myelogenous leukemia and renal cell cancer. There remains much to learn, but the future is bright for anti-AXL therapies, though effective combinations and their impact may not be realized for years to come. Clin Cancer Res; 23(12); 2928-33. ©2017 AACR.
©2017 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Robert C, Thomas L, Bondarenko I, O’Day S, Weber J, Garbe C, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. The New England journal of medicine. 2011;364(26):2517–26. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
