

Continuum of Renin-Independent Aldosteronism in Normotension
- PMID: 28289182
- PMCID: PMC5391287
- DOI: 10.1161/HYPERTENSIONAHA.116.08952
Continuum of Renin-Independent Aldosteronism in Normotension
Abstract
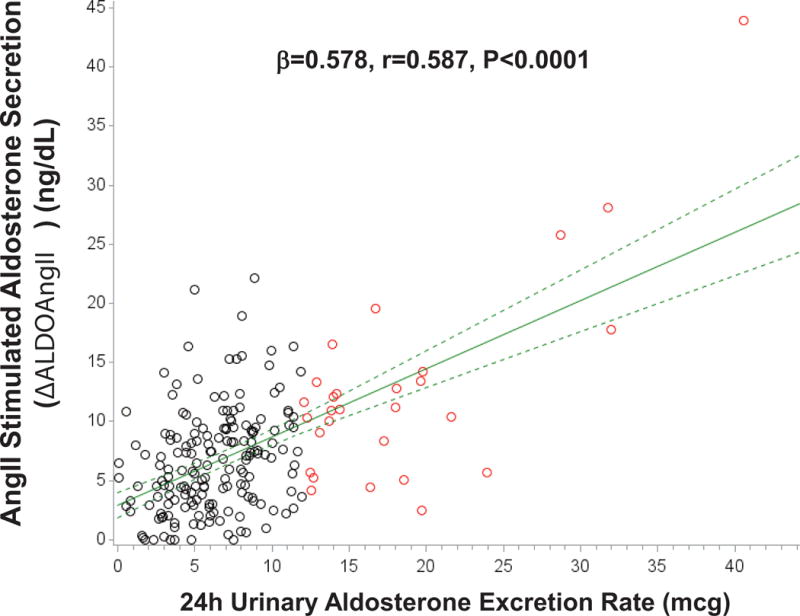
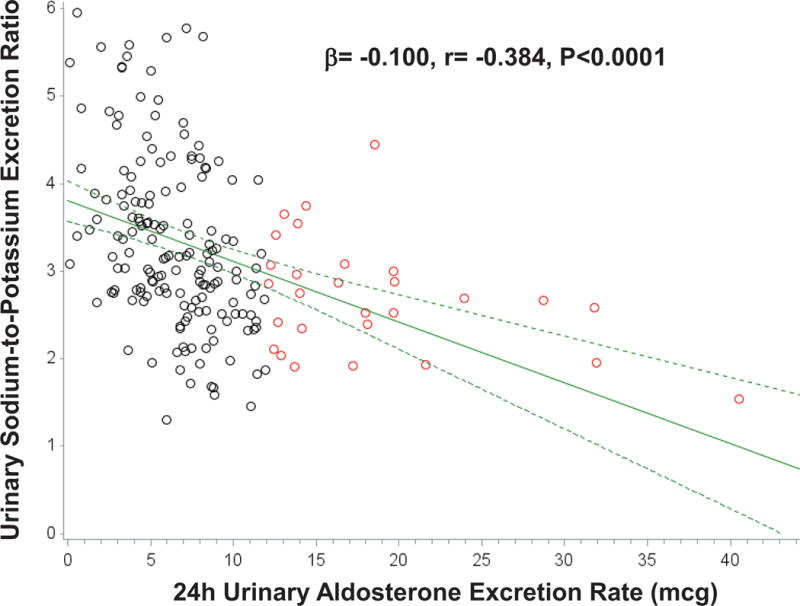
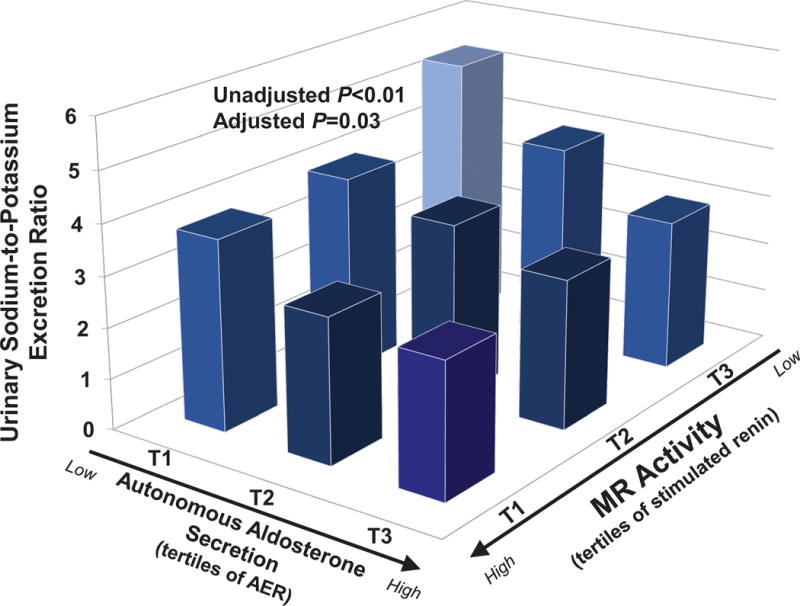
Primary aldosteronism is a severe form of autonomous aldosteronism. Milder forms of autonomous and renin-independent aldosteronism may be common, even in normotension. We characterized aldosterone secretion in 210 normotensives who had suppressed plasma renin activity (<1.0 ng/mL per hour), completed an oral sodium suppression test, received an infusion of angiotensin II, and had measurements of blood pressure and renal plasma flow. Continuous associations between urinary aldosterone excretion rate, renin, and potassium handling were investigated. Severe autonomous aldosterone secretion that was consistent with confirmed primary aldosteronism was defined based on accepted criteria of an aldosterone excretion rate >12 μg/24 hours with urinary sodium excretion >200 mmol/24 hours. Across the population, there were strong and significant associations between higher aldosterone excretion rate and higher urinary potassium excretion, higher angiotensin II-stimulated aldosterone, and lower plasma renin activity, suggesting a continuum of renin-independent aldosteronism and mineralocorticoid receptor activity. Autonomous aldosterone secretion that fulfilled confirmatory criteria for primary aldosteronism was detected in 29 participants (14%). Normotensives with evidence suggestive of confirmed primary aldosteronism had higher 24-hour urinary aldosterone excretion rate (20.2±12.2 versus 6.2±2.9 μg/24 hours; P<0.001) as expected, but also higher angiotensin II-stimulated aldosterone (12.4±8.6 versus 6.6±4.3 ng/dL; P<0.001) and lower 24-hour urinary sodium-to-potassium excretion (2.69±0.65 versus 3.69±1.50 mmol/mmol; P=0.001); however, there were no differences in age, aldosterone-to-renin ratio, blood pressure, or renal plasma flow between the 2 groups. These findings indicate a continuum of renin-independent aldosteronism and mineralocorticoid receptor activity in normotension that ranges from subtle to overtly dysregulated and autonomous. Longitudinal studies are needed to determine whether this spectrum of autonomous aldosterone secretion contributes to hypertension and cardiovascular disease.
Keywords: aldosterone; hypertension; normotensive; potassium; primary aldosteronism; renin.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
Primary Aldosteronism or Not Primary Aldosteronism: Is This Now the Question in Normotension?Hypertension. 2017 May;69(5):780-781. doi: 10.1161/HYPERTENSIONAHA.117.09050. Epub 2017 Mar 13. Hypertension. 2017. PMID: 28289179 No abstract available.
References
-
- Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H, Stowasser M, Young WF., Jr The management of primary aldosteronism: Case detection, diagnosis, and treatment: An endocrine society clinical practice guideline. The Journal of Clinical Endocrinology and Metabolism. 2016;101:1889–1916. - PubMed
-
- Piaditis G, Markou A, Papanastasiou L, Androulakis II, Kaltsas G. Progress in aldosteronism: A review of the prevalence of primary aldosteronism in pre-hypertension and hypertension. European Journal of Endocrinology. 2015;172:R191–203. - PubMed
-
- Mosso L, Carvajal C, Gonzalez A, Barraza A, Avila F, Montero J, Huete A, Gederlini A, Fardella CE. Primary aldosteronism and hypertensive disease. Hypertension. 2003;42:161–165. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
