

Antimalarial Drug Resistance: A Threat to Malaria Elimination
- PMID: 28289248
- PMCID: PMC5495053
- DOI: 10.1101/cshperspect.a025619
Antimalarial Drug Resistance: A Threat to Malaria Elimination
Abstract
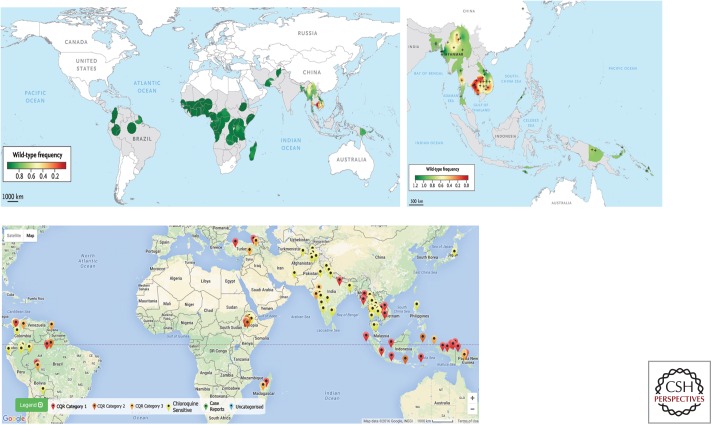
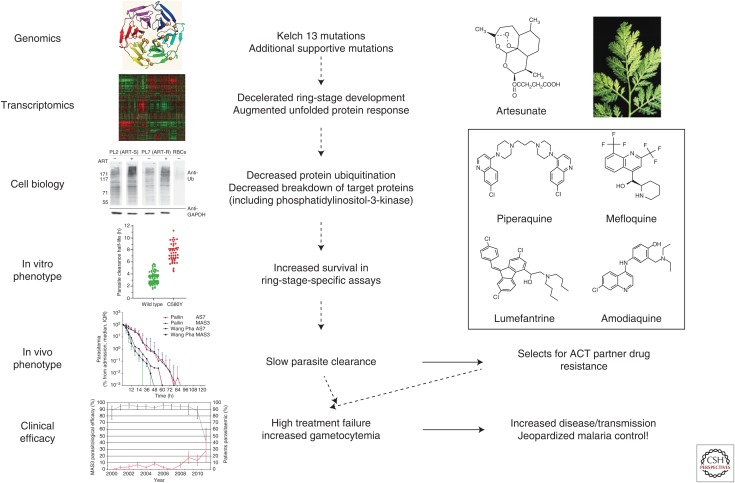
Increasing antimalarial drug resistance once again threatens effective antimalarial drug treatment, malaria control, and elimination. Artemisinin combination therapies (ACTs) are first-line treatment for uncomplicated falciparum malaria in all endemic countries, yet partial resistance to artemisinins has emerged in the Greater Mekong Subregion. Concomitant emergence of partner drug resistance is now causing high ACT treatment failure rates in several areas. Genetic markers for artemisinin resistance and several of the partner drugs have been established, greatly facilitating surveillance. Single point mutations in the gene coding for the Kelch propeller domain of the K13 protein strongly correlate with artemisinin resistance. Novel regimens and strategies using existing antimalarial drugs will be needed until novel compounds can be deployed. Elimination of artemisinin resistance will imply elimination of all falciparum malaria from the same areas. In vivax malaria, chloroquine resistance is an increasing problem.
Copyright © 2017 Cold Spring Harbor Laboratory Press; all rights reserved.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials