

Ivabradine in the treatment of systolic heart failure - A systematic review and meta-analysis
- PMID: 28289533
- PMCID: PMC5329746
- DOI: 10.4330/wjc.v9.i2.182
Ivabradine in the treatment of systolic heart failure - A systematic review and meta-analysis
Abstract
Aim: To perform a systematic-review and meta-analysis to compare outcomes of ivabradine combined with beta-blocker to beta-blocker alone in heart failure with reduced ejection fraction (HFrEF).
Methods: We searched PubMed, Cochrane, EMBASE, CINAHL and Web of Science for trials comparing ivabradine + beta-blocker to beta-blocker alone in HFrEF. We performed a systematic-review and meta-analysis of published literature. Primary end-point was combined end point of cardiac death and hospitalization for heart failure.
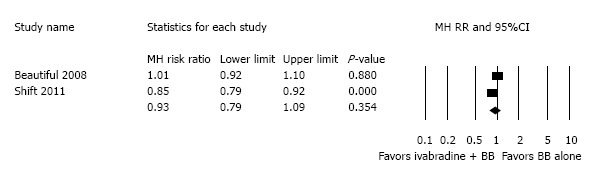
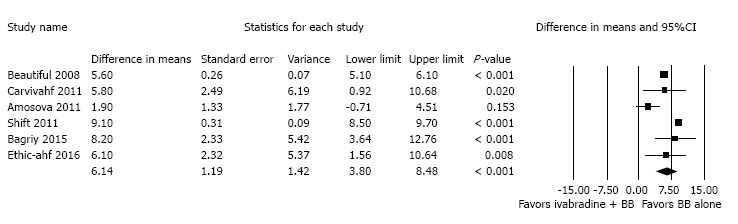
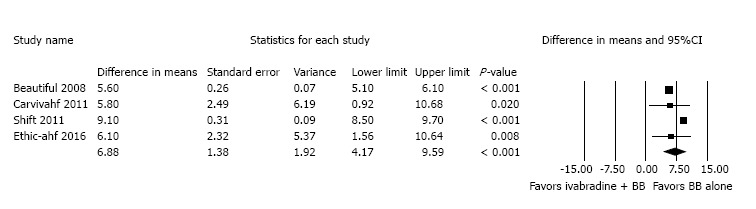
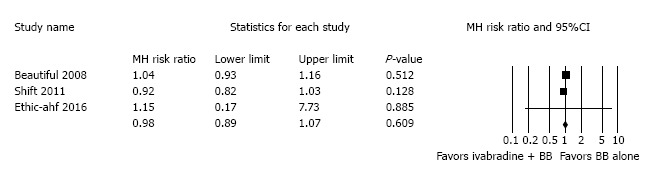
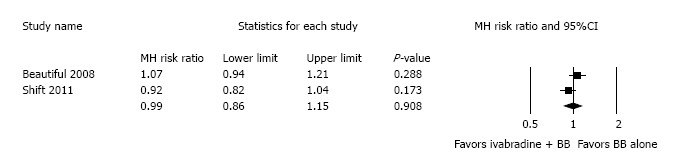
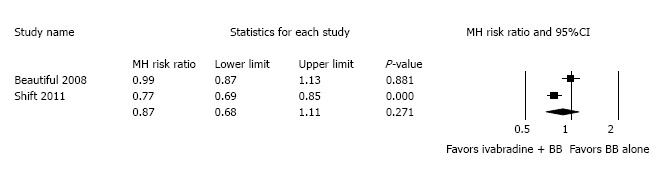
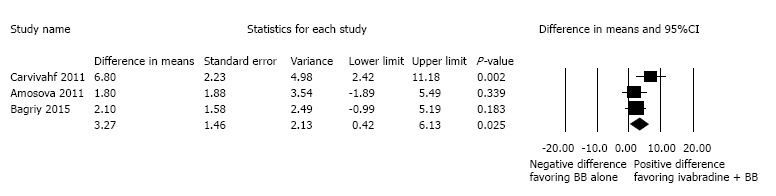
Results: Six studies with 17671 patients were included. Mean follow-up was 8.7 ± 7.9 mo. Combined end-point of heart failure readmission and cardiovascular death was better in ivabradine + beta-blocker group compared to beta-blocker alone (RR: 0.93, 95%CI: 0.79-1.09, P = 0.354). Mean difference (MD) in heart rate was higher in the ivabradine + beta-blocker group (MD: 6.14, 95%CI: 3.80-8.48, P < 0.001). There was no difference in all cause mortality (RR: 0.98, 95%CI: 0.89-1.07, P = 0.609), cardiovascular mortality (RR: 0.99, 95%CI: 0.86-1.15, P = 0.908) or heart failure hospitalization (RR: 0.87, 95%CI: 0.68-1.11, P = 0.271).
Conclusion: From the available clinical trials, ivabradine + beta-blocker resulted in a significantly greater reduction in HR coupled with improvement in combined end-point of heart failure readmission and cardiovascular death but with no improvement in all cause or cardiovascular mortality. Given the limited evidence, further randomized controlled trials are essential before widespread clinical application of ivabradine + beta-blocker is advocated for HFrEF.
Keywords: Heart failure; Ivabradine.
Conflict of interest statement
Conflict-of-interest statement: Drs. Mahesh Anantha Narayanan, Yogesh N Reddy, Janani Baskaran and Ganesh Raveendran have no disclosures; Dr. Benditt is a consultant for and holds equity in Medtronic Inc., and St Jude Medical Inc. Dr. Benditt is supported in part by a grant from the Dr. Earl E Bakken Family in support of heart-brain research.
Figures
References
-
- Crespo-Leiro MG, Anker SD, Maggioni AP, Coats AJ, Filippatos G, Ruschitzka F, Ferrari R, Piepoli MF, Delgado Jimenez JF, Metra M, et al. European Society of Cardiology Heart Failure Long-Term Registry (ESC-HF-LT): 1-year follow-up outcomes and differences across regions. Eur J Heart Fail. 2016;18:613–625. - PubMed
-
- McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, Falk V, Filippatos G, Fonseca C, Gomez-Sanchez MA, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012;14:803–869. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:e147–e239. - PubMed
-
- Böhm M, Swedberg K, Komajda M, Borer JS, Ford I, Dubost-Brama A, Lerebours G, Tavazzi L. Heart rate as a risk factor in chronic heart failure (SHIFT): the association between heart rate and outcomes in a randomised placebo-controlled trial. Lancet. 2010;376:886–894. - PubMed
-
- Fox K, Borer JS, Camm AJ, Danchin N, Ferrari R, Lopez Sendon JL, Steg PG, Tardif JC, Tavazzi L, Tendera M. Resting heart rate in cardiovascular disease. J Am Coll Cardiol. 2007;50:823–830. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
