

Acid-base disturbances in nephrotic syndrome: analysis using the CO2/HCO3 method (traditional Boston model) and the physicochemical method (Stewart model)
- PMID: 28289910
- PMCID: PMC5648741
- DOI: 10.1007/s10157-017-1387-8
Acid-base disturbances in nephrotic syndrome: analysis using the CO2/HCO3 method (traditional Boston model) and the physicochemical method (Stewart model)
Abstract
Background: The Stewart model for analyzing acid-base disturbances emphasizes serum albumin levels, which are ignored in the traditional Boston model. We compared data derived using the Stewart model to those using the Boston model in patients with nephrotic syndrome.
Methods: Twenty-nine patients with nephrotic syndrome and six patients without urinary protein or acid-base disturbances provided blood and urine samples for analysis that included routine biochemical and arterial blood gas tests, plasma renin activity, and aldosterone. The total concentration of non-volatile weak acids (ATOT), apparent strong ion difference (SIDa), effective strong ion difference (SIDe), and strong ion gap (SIG) were calculated according to the formulas of Agrafiotis in the Stewart model.
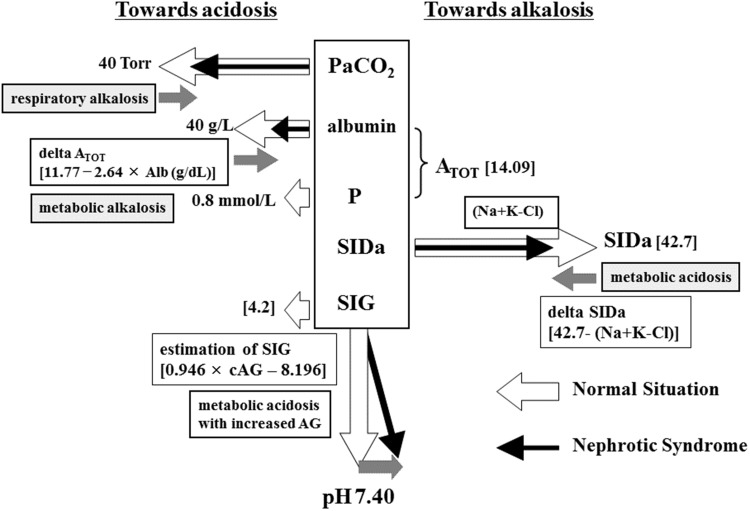
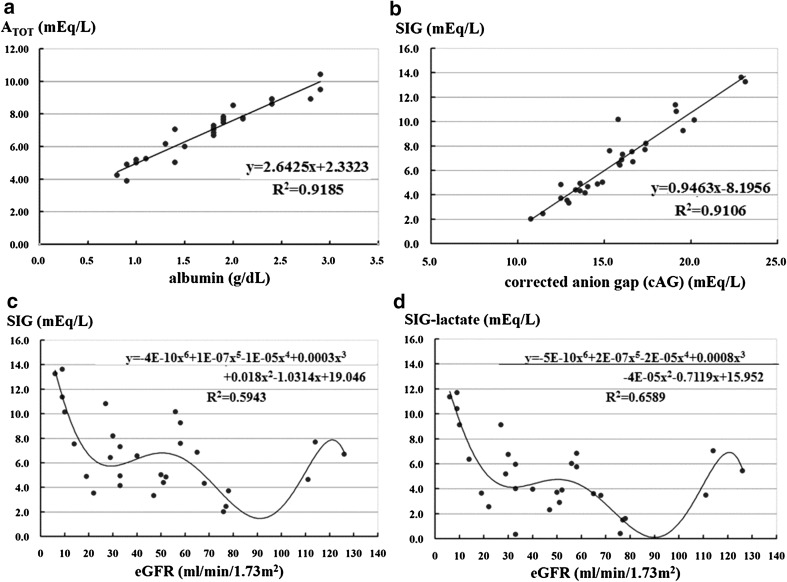
Results: According to the Boston model, 25 of 29 patients (90%) had alkalemia. Eighteen patients had respiratory alkalosis, 11 had metabolic alkalosis, and 4 had both conditions. Only three patients had hyperreninemic hyperaldosteronism. The Stewart model demonstrated respiratory alkalosis based on decreased PaCO2, metabolic alkalosis based on decreased ATOT, and metabolic acidosis based on decreased SIDa. We could diagnose metabolic alkalosis or acidosis with a normal anion gap after comparing delta ATOT [(14.09 - measured ATOT) or (11.77 - 2.64 × Alb (g/dL))] and delta SIDa [(42.7 - measured SIDa) or (42.7 - (Na + K - Cl)]). We could also identify metabolic acidosis with an increased anion gap using SIG > 7.0 (SIG = 0.9463 × corrected anion gap-8.1956).
Conclusions: Patients with nephrotic syndrome had primary respiratory alkalosis, decreased ATOT due to hypoalbuminemia (power to metabolic alkalosis), and decreased levels of SIDa (power to metabolic acidosis). We could detect metabolic acidosis with an increased anion gap by calculating SIG. The Stewart model in combination with the Boston model facilitates the analysis of complex acid-base disturbances in nephrotic syndrome.
Keywords: Acid–base disturbance; Metabolic acidosis; Nephrotic syndrome; Renin–angiotensin–aldosterone system; Respiratory alkalosis.
Conflict of interest statement
Conflict of interest
The authors have declared that no conflict of interest exists.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee at which the studies were conducted (Aichi Medical University 14-164) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
