

Magnetic resonance spectroscopic analysis of multifidus muscles lipid content and association with spinopelvic malalignment in chronic low back pain
- PMID: 28291378
- PMCID: PMC5605103
- DOI: 10.1259/bjr.20160753
Magnetic resonance spectroscopic analysis of multifidus muscles lipid content and association with spinopelvic malalignment in chronic low back pain
Abstract
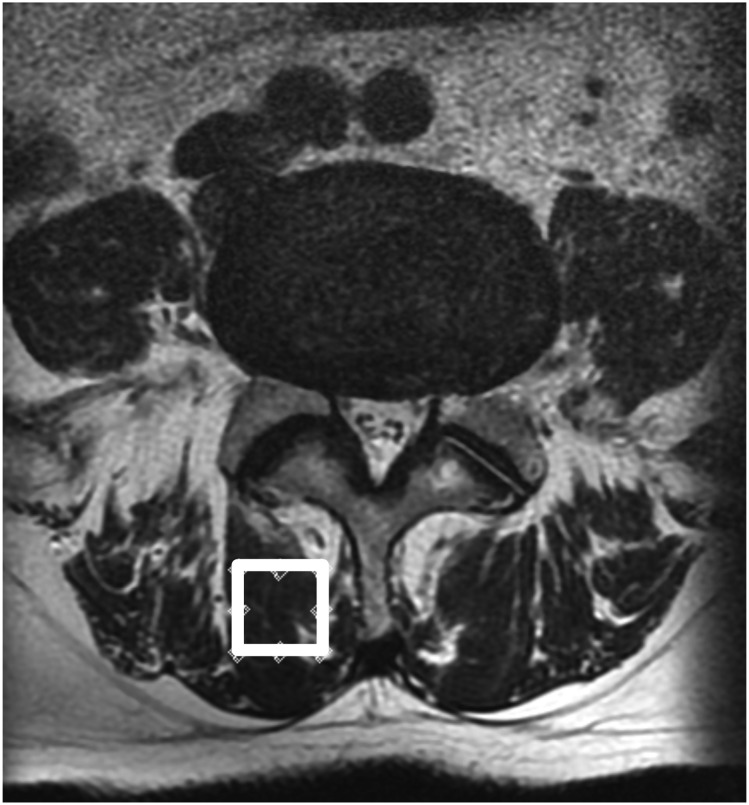
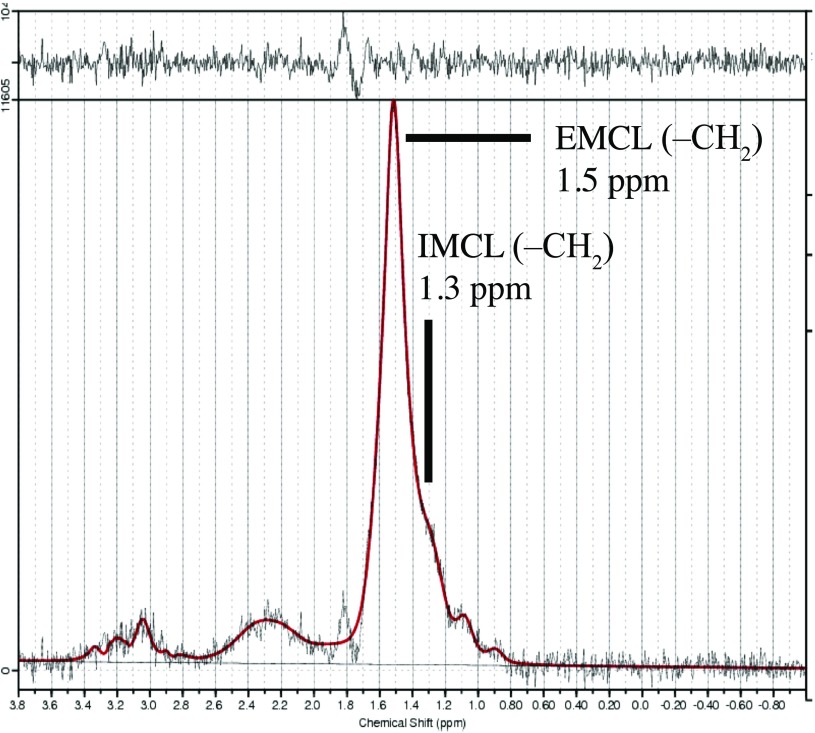
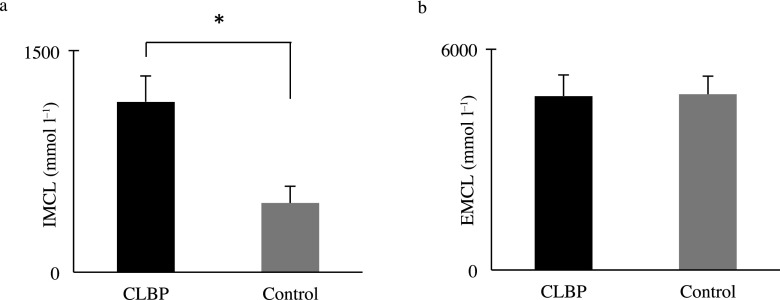
Objective: To analyze intramyocellular lipids (IMCLs) and extramyocellular lipids (EMCLs) of the multifidus muscle (Mm) using MR spectroscopy in chronic low back pain (CLBP) and control groups and to identify correlations with spinopelvic alignment.
Methods: 40 patients (16 males, 24 females; mean age, 62.9 ± 1.9 years) whose visual analogue scale scores were >30 mm for CLBP were included. Furthermore, 40 control participants matched with the CLBP group subjects by sample size, gender and age (17 males, 23 females; mean age, 65.0 ± 1.2 years) were included. We compared the body mass index, physical workload, leisure time physical activity level, spinopelvic parameters, and IMCLs and EMCLs of the Mm between the groups. We also evaluated possible correlations of spinopelvic parameters with IMCLs and EMCLs of the Mm in the groups.
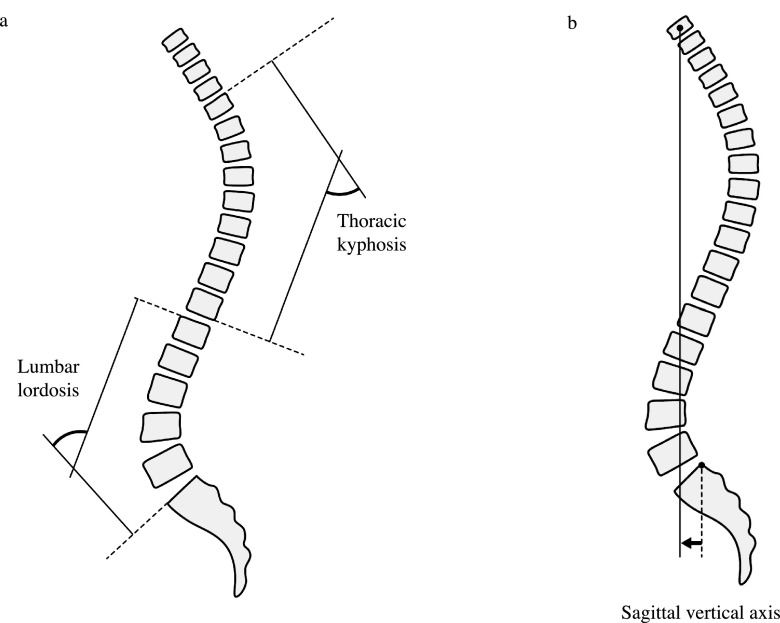
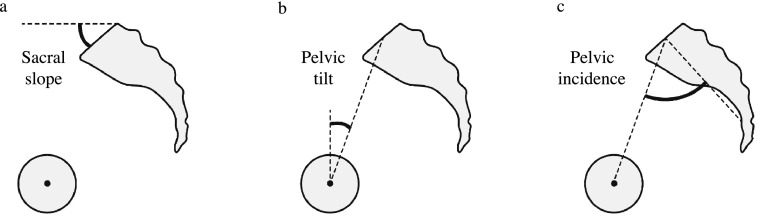
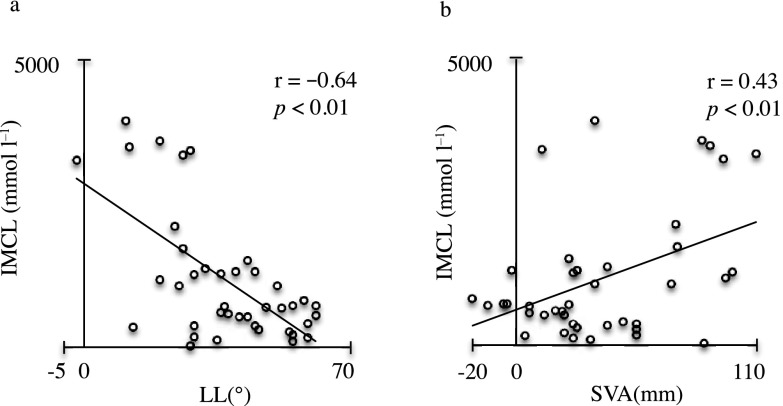
Results: There were no statistically significant differences in body mass index, physical workload, exercise intensity level, spinopelvic parameters and EMCLs between the groups. The IMCLs were significantly higher in the CLBP group than in the control group (p < 0.01). In the CLBP group, there was a significantly negative correlation between IMCLs and lumbar lordosis (r = -0.64, p < 0.01) and a significantly positive correlation between IMCLs and sagittal vertical axis (r = 0.43, p < 0.01).
Conclusion: The measurement of IMCLs might be a characteristic finding of CLBP as well as a precursor to spinal deformity. Advances in knowledge: IMCLs of the Mm may be a useful prognostic marker in rehabilitation strategies for patients with CLBP.
Figures
References
-
- Deyo RA, Weinstein JN. Low back pain. N Engl J Med 2001; 344: 363–70. doi: https://doi.org/10.1056/NEJM200102013440508 - DOI - PubMed
-
- Hurwitz EL, Morgenstern H. The effects of comorbidity and other factors on medical versus chiropractic care for back problems. Spine (Phila Pa 1976) 1997; 22: 2254–63; discussion 2263–4. - PubMed
-
- Shekelle PG, Markovich M, Louie R. An epidemiologic study of episodes of back pain care. Spine (Phila Pa 1976) 1995; 20: 1668–73. - PubMed
-
- Balague F, Mannion AF, Pellise F, Cedraschi C. Non-specific low back pain. Lancet 2012; 379: 482–91. - PubMed
-
- Cholewicki J, Panjabi MM, Khachatryan A. Stabilizing function of trunk flexor-extensor muscles around a neutral spine posture. Spine (Phila Pa 1976) 1997; 22: 2207–12. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
