

Therapy for Relapsed Multiple Myeloma: Guidelines From the Mayo Stratification for Myeloma and Risk-Adapted Therapy
- PMID: 28291589
- PMCID: PMC5554888
- DOI: 10.1016/j.mayocp.2017.01.003
Therapy for Relapsed Multiple Myeloma: Guidelines From the Mayo Stratification for Myeloma and Risk-Adapted Therapy
Abstract
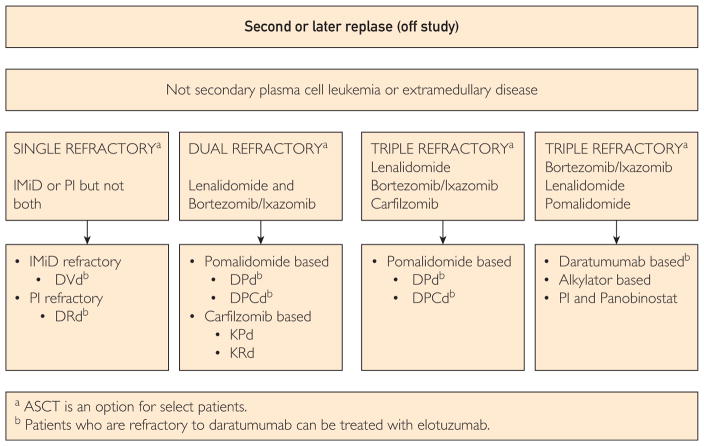
Life expectancy in patients with multiple myeloma is increasing because of the availability of an increasing number of novel agents with various mechanisms of action against the disease. However, the disease remains incurable in most patients because of the emergence of resistant clones, leading to repeated relapses of the disease. In 2015, 5 novel agents were approved for therapy for relapsed multiple myeloma. This surfeit of novel agents renders management of relapsed multiple myeloma more complex because of the occurrence of multiple relapses, the risk of cumulative and emergent toxicity from previous therapies, as well as evolution of the disease during therapy. A group of physicians at Mayo Clinic with expertise in the care of patients with multiple myeloma regularly evaluates the evolving literature on the biology and therapy for multiple myeloma and issues guidelines on the optimal care of patients with this disease. In this article, the latest recommendations on the diagnostic evaluation of relapsed multiple myeloma and decision trees on how to treat patients at various stages of their relapse (off study) are provided together with the evidence to support them.
Copyright © 2017 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures




References
-
- Shaughnessy JD, Jr, Zhan F, Burington BE, et al. A validated gene expression model of high-risk multiple myeloma is defined by deregulated expression of genes mapping to chromosome 1. Blood. 2007;109(6):2276–2284. - PubMed
-
- Avet-Loiseau H, Attal M, Moreau P, et al. Genetic abnormalities and survival in multiple myeloma: the experience of the Intergroupe Francophone du Myélome. Blood. 2007;109(8):3489–3495. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
