

Impact of a structured ICU training programme in resource-limited settings in Asia
- PMID: 28291809
- PMCID: PMC5349661
- DOI: 10.1371/journal.pone.0173483
Impact of a structured ICU training programme in resource-limited settings in Asia
Abstract
Objective: To assess the impact on ICU performance of a modular training program in three resource-limited general adult ICUs in India, Bangladesh, and Nepal.
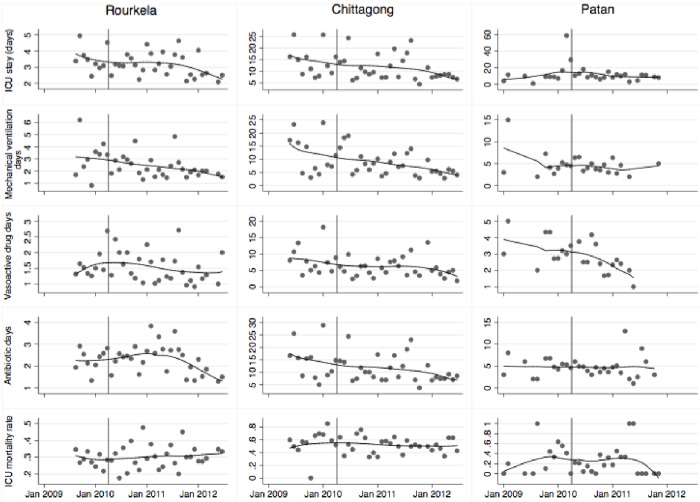
Method: A modular ICU training programme was evaluated using performance indicators from June 2009 to June 2012 using an interrupted time series design with an 8 to 15 month pre-intervention and 18 to 24 month post-intervention period. ICU physicians and nurses trained in Europe and the USA provided training for ICU doctors and nurses. The training program consisted of six modules on basic intensive care practices of 2-3 weeks each over 20 months. The performance indicators consisting of ICU mortality, time to ICU discharge, rate at which patients were discharged alive from the ICU, discontinuation of mechanical ventilation or vasoactive drugs and duration of antibiotic use were extracted. Stepwise changes and changes in trends associated with the intervention were analysed.
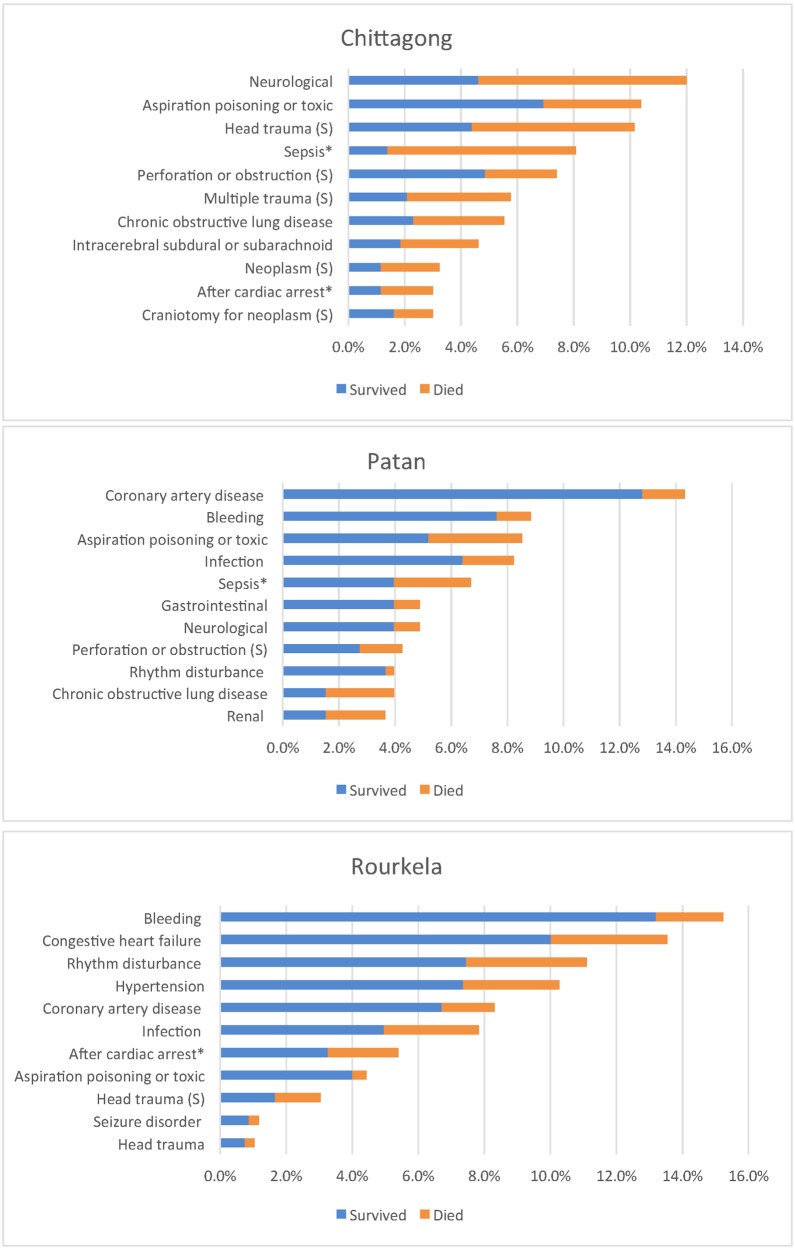
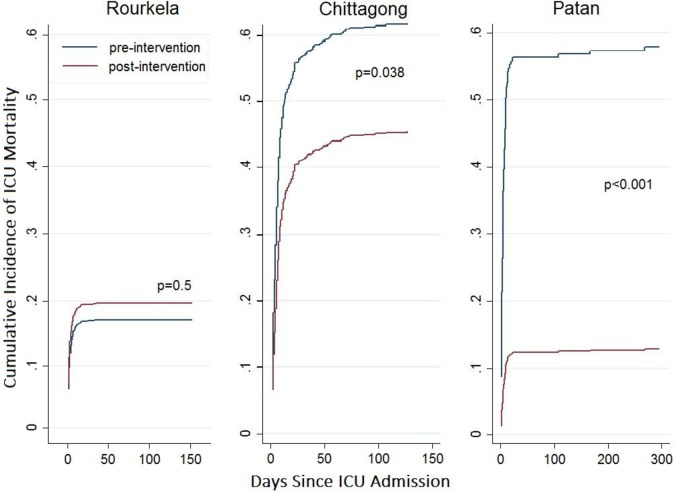
Results: Pre-Training ICU mortality in Rourkela (India), and Patan (Nepal) Chittagong (Bangladesh), was 28%, 41% and 62%, respectively, compared to 30%, 18% and 51% post-intervention. The intervention was associated with a stepwise reduction in cumulative incidence of in-ICU mortality in Chittagong (adjusted subdistribution hazard ratio [aSHR] (95% CI): 0.62 (0.40, 0.97), p = 0.03) and Patan (aSHR 0.16 (0.06, 0.41), p<0.001), but not in Rourkela (aSHR: 1.17 (0.75, 1.82), p = 0.49). The intervention was associated with earlier discontinuation of vasoactive drugs at Rourkela (adjusted hazard ratio for weekly change [aHR] 1.08 (1.03, 1.14), earlier discontinuation of mechanical ventilation in Chittagong (aHR 2.97 (1.24, 7.14), p = 0.02), and earlier ICU discharge in Patan (aHR 1.87 (1.02, 3.43), p = 0.04).
Conclusion: This structured training program was associated with a decrease in ICU mortality in two of three sites and improvement of other performance indicators. A larger cluster randomised study assessing process outcomes and longer-term indicators is warranted.
Conflict of interest statement
Figures
References
-
- Haniffa R, Dondorp A. A cross sectional survey of critical care services in Sri Lanka; a low-middle income country. J Crit Care. 2014; - PubMed
-
- Adhikari NK, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical care and the global burden of critical illness in adults. Lancet. Interdepartmental Division of Critical Care, University of Toronto and Department of Critical Care Medicine, Sunnybrook Health Sciences Centre, Toronto, ON, Canada.; 2010. October;376(9749):1339–46. 10.1016/S0140-6736(10)60446-1 - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
