

Unwarranted Variation in the Quality of Care for Patients With Diseases of the Thoracic Aorta
- PMID: 28292748
- PMCID: PMC5524021
- DOI: 10.1161/JAHA.116.004913
Unwarranted Variation in the Quality of Care for Patients With Diseases of the Thoracic Aorta
Abstract
Background: Thoracic aortic disease has a high mortality. We sought to establish the contribution of unwarranted variation in care to regional differences in outcomes observed in patients with thoracic aortic disease in England.
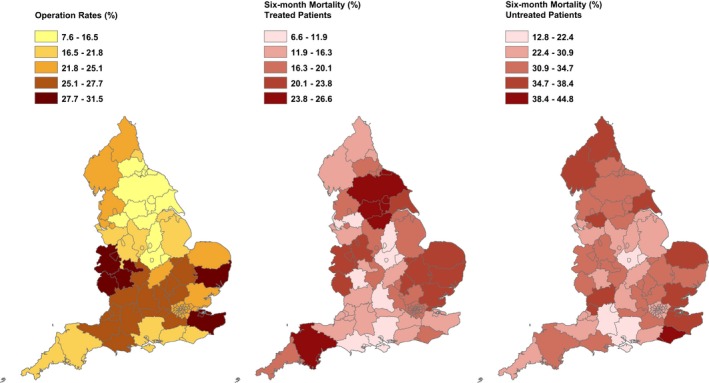
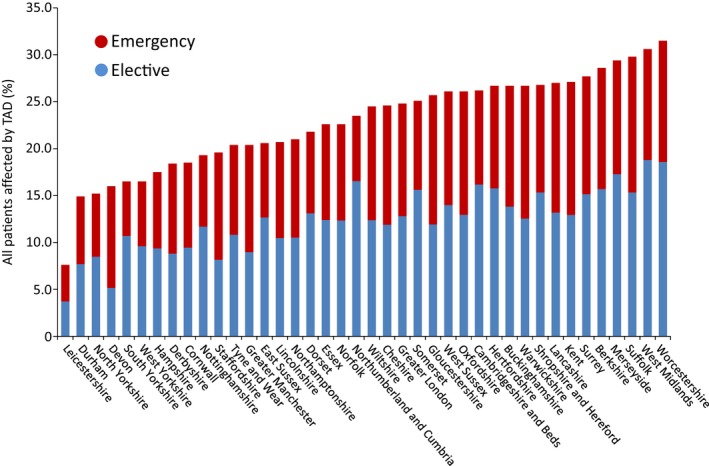
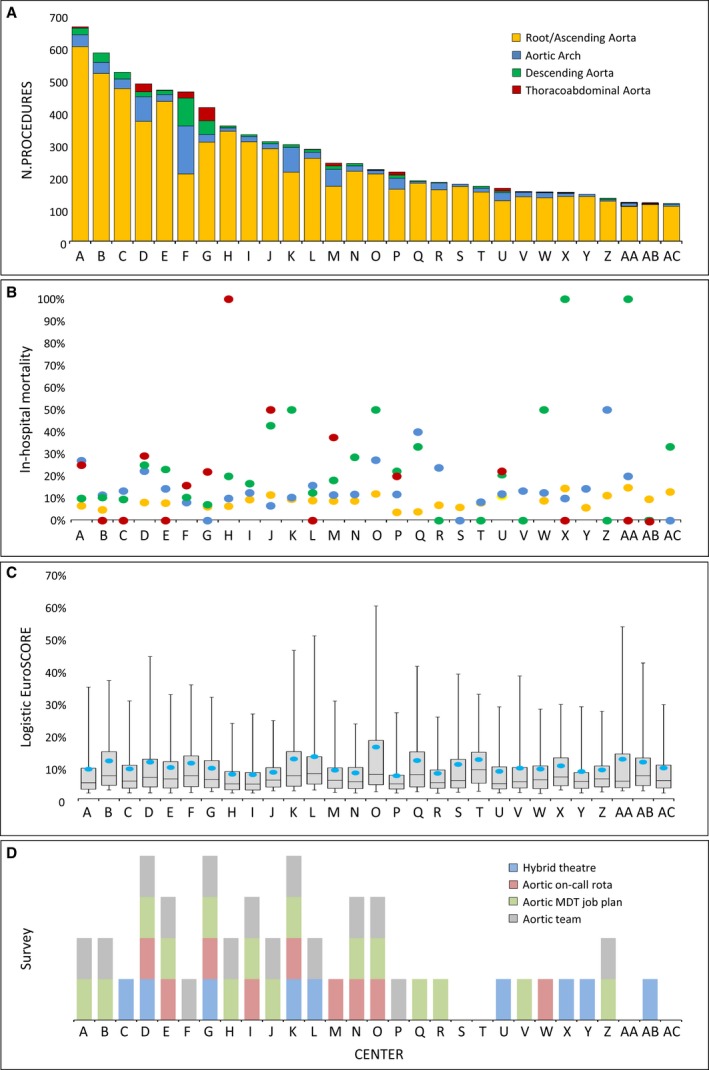
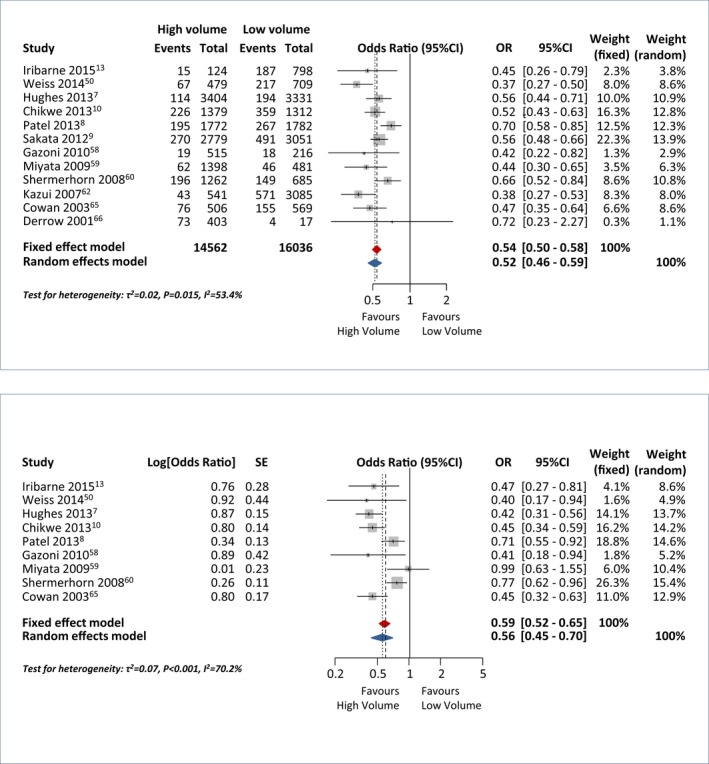
Methods and results: Data from the Hospital Episode Statistics (HES) and the National Adult Cardiac Surgery Audit (NACSA) were extracted. A parallel systematic review/meta-analysis through December 2015, and structure and process questionnaire of English cardiac surgery units were also accomplished. Treatment and mortality rates were investigated. A total of 24 548 adult patients in the HES study, 8058 in the NACSA study, and 103 543 from a total of 33 studies in the systematic review were obtained. Treatment rates for thoracic aortic disease within 6 months of index admission ranged from 7.6% to 31.5% between English counties. Risk-adjusted 6-month mortality in untreated patients ranged from 19.4% to 36.3%. Regional variation persisted after adjustment for disease or patient factors. Regional cardiac units with higher case volumes treated more-complex patients and had significantly lower risk-adjusted mortality relative to low-volume units. The results of the systematic review indicated that the delivery of care by multidisciplinary teams in high-volume units resulted in better outcomes. The observational analyses and the online survey indicated that this is not how services are configured in most units in England.
Conclusions: Changes in the organization of services that address unwarranted variation in the provision of care for patients with thoracic aortic disease in England may result in more-equitable access to treatment and improved outcomes.
Keywords: aortic disease; aortic dissection; cardiac surgery; quality of care.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Sampson UK, Norman PE, Fowkes FG, Aboyans V, Yanna Song, Harrell FE Jr, Forouzanfar MH, Naghavi M, Denenberg JO, McDermott MM, Criqui MH, Mensah GA, Ezzati M, Murray C. Global and regional burden of aortic dissection and aneurysms: mortality trends in 21 world regions, 1990 to 2010. Glob Heart. 2014;9:171–180. - PubMed
-
- Olsson C, Thelin S, Ståhle E, Ekbom A, Granath F. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population‐based study of more than 14,000 cases from 1987 to 2002. Circulation. 2006;114:2611–2618. - PubMed
-
- von Allmen RS, Anjum A, Powell JT. Incidence of descending aortic pathology and evaluation of the impact of thoracic endovascular aortic repair: a population‐based study in England and Wales from 1999 to 2010. Eur J Vasc Endovasc Surg. 2013;45:154–159. - PubMed
-
- Raghupathy A, Nienaber CA, Harris KM, Myrmel T, Fattori R, Sechtem U, Oh J, Trimarchi S, Cooper JV, Booher A, Eagle K, Isselbacher E, Bossone E; International Registry of Acute Aortic Dissection (IRAD) Investigators . Geographic differences in clinical presentation, treatment, and outcomes in type A acute aortic dissection (from the International Registry of Acute Aortic Dissection). Am J Cardiol. 2008;102:1562–1566. - PubMed
-
- Liao JM, Bakaeen FG, Cornwell LD, Simpson K, Lemaire SA, Coselli JS, Chu D. Nationwide trends and regional/hospital variations in open versus endovascular repair of thoracoabdominal aortic aneurysms. J Thorac Cardiovasc Surg. 2012;144:612–616. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
