

Effectiveness of combined macular buckle under direct vision and vitrectomy with ILM peeling in refractory macular hole retinal detachment with extreme high axial myopia: a 24-month comparative study
- PMID: 28292775
- PMCID: PMC5629954
- DOI: 10.1136/bjophthalmol-2016-310123
Effectiveness of combined macular buckle under direct vision and vitrectomy with ILM peeling in refractory macular hole retinal detachment with extreme high axial myopia: a 24-month comparative study
Abstract
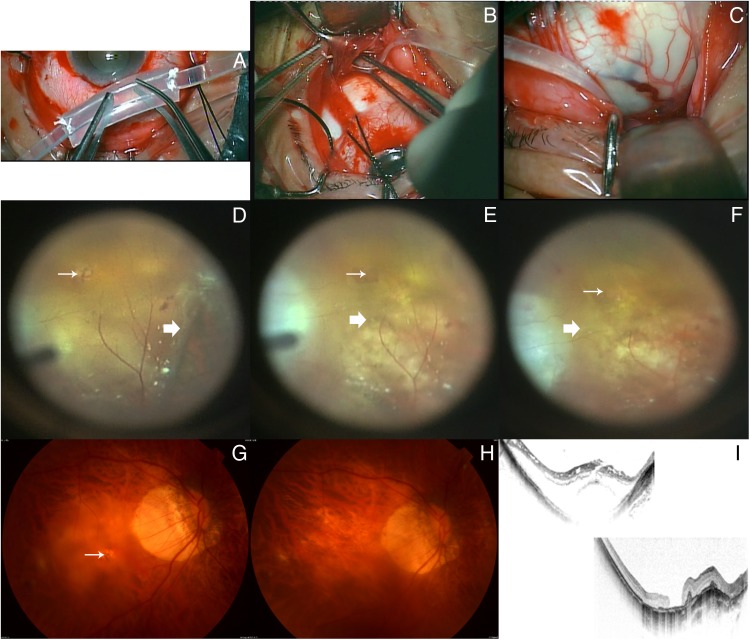
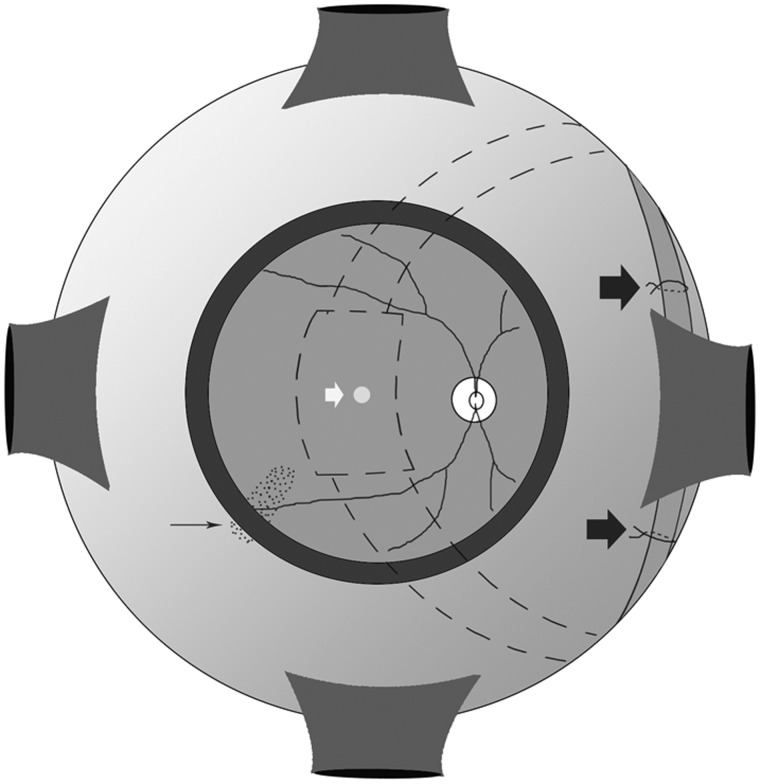
Purpose: To evaluate the efficacy of a combined macular buckle under direct vision and 23-gauge pars plana vitrectomy (PPV) with internal limiting membrane (ILM) peeling in refractory macular hole retinal detachment (MHRD) with extreme high axial myopia.
Design: Prospective, randomised controlled study.
Participants: The study included 98 eyes of 98 patients of MHRD with extreme high axial (>30 mm) myopia.
Intervention: Patients were randomly assigned to undergo PPV with ILM peeling (group 1, n=52) or PPV with ILM peeling combined with macular buckle under direct vision (group 2, n=46).
Main outcome measures: Complete ocular examination included best-corrected visual acuity (BCVA) (LogMAR), applanation tonometry, optical biometry, slit-lamp biomicroscopy, colour fundus photography, ultrasound examination and optical coherence tomography at baseline and every follow-up visit.
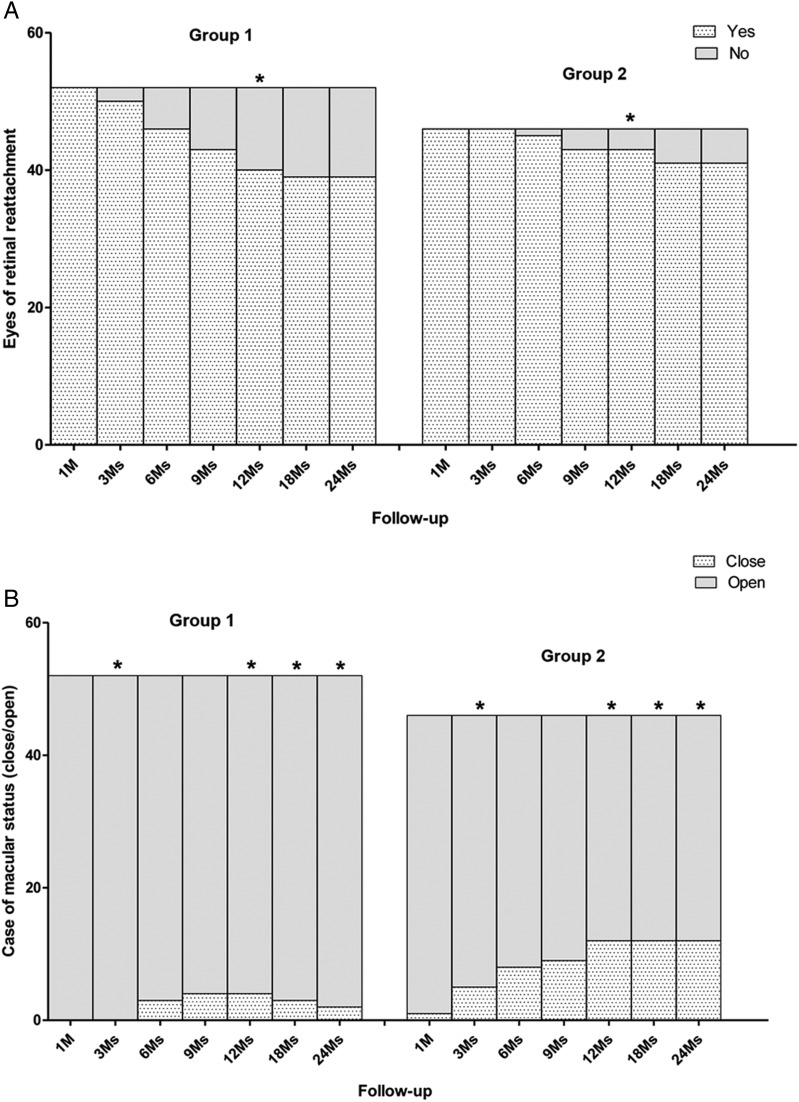
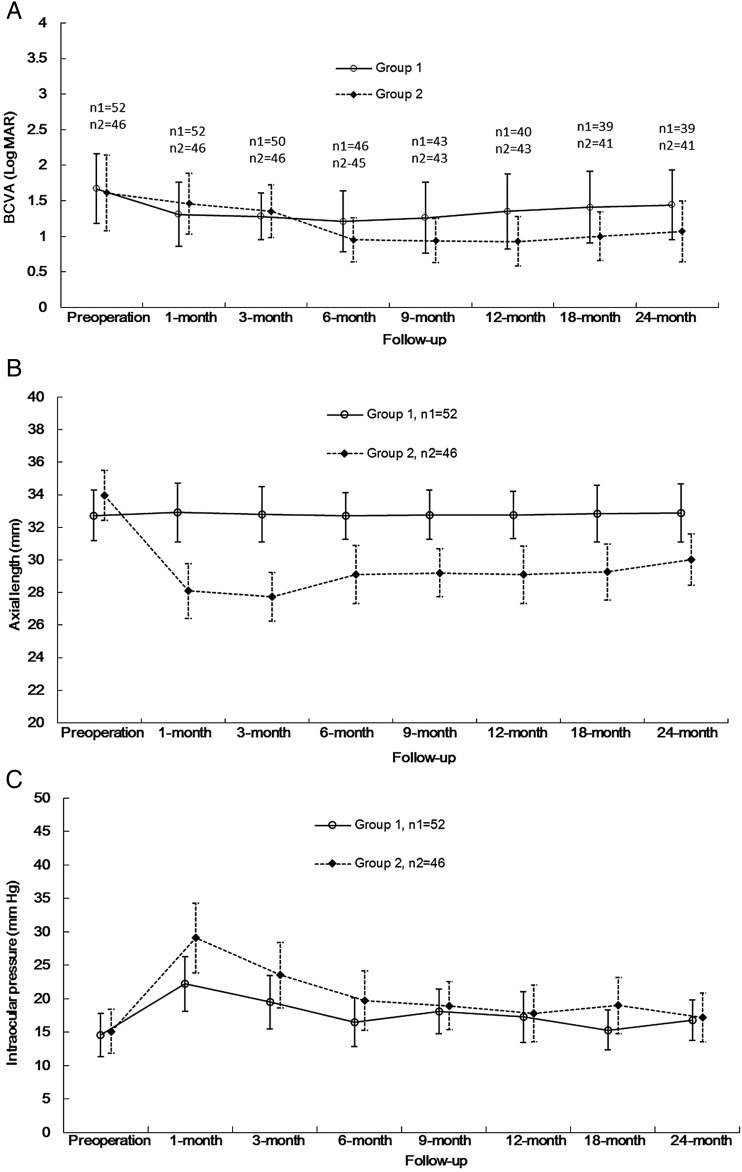
Results: Initial retinal reattachment rate was significantly higher in group 2 than in group 1 at 12-month postoperatively (χ2 test, p=0.020). Macular hole closure rate in group 2 was significantly higher than that in group 1 at 3, 12, 18 and 24 months postoperatively (Fisher's exact test, p<0.05). In initial retinal reattachment cases, the mean BCVA decreased significantly in group 2 than in group 1 at 3 months postoperatively (Wilcoxon matched pairs signed rank test, p=0.036), and had increased significantly in group 2 than in group 1 since 6 months postoperatively (Wilcoxon matched pairs signed rank test, p<0.05). Mean axial lengths in group 2 were significantly shorter than that of group 1 at each follow-up time point (Wilcoxon matched pairs signed rank test, p<0.05).
Conclusions: Combined macular buckle under direct vision and PPV with ILM peeling is more effective in treatment of MHRD with extreme high axial (>30 mm) myopia.
Keywords: Macula; Retina.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous