

18F-Fluoride and 18F-Fluorodeoxyglucose Positron Emission Tomography After Transient Ischemic Attack or Minor Ischemic Stroke: Case-Control Study
- PMID: 28292859
- PMCID: PMC5367506
- DOI: 10.1161/CIRCIMAGING.116.004976
18F-Fluoride and 18F-Fluorodeoxyglucose Positron Emission Tomography After Transient Ischemic Attack or Minor Ischemic Stroke: Case-Control Study
Abstract
Background: Combined positron emission tomography (PET) and computed tomography (CT) can assess both anatomy and biology of carotid atherosclerosis. We sought to assess whether 18F-fluoride or 18F-fluorodeoxyglucose can identify culprit and high-risk carotid plaque.
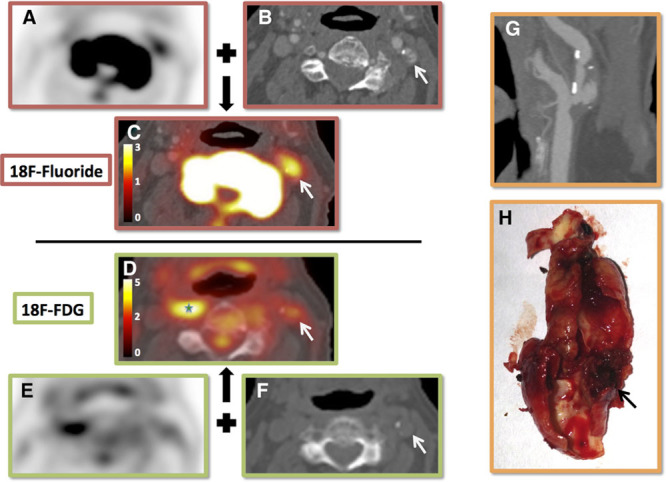
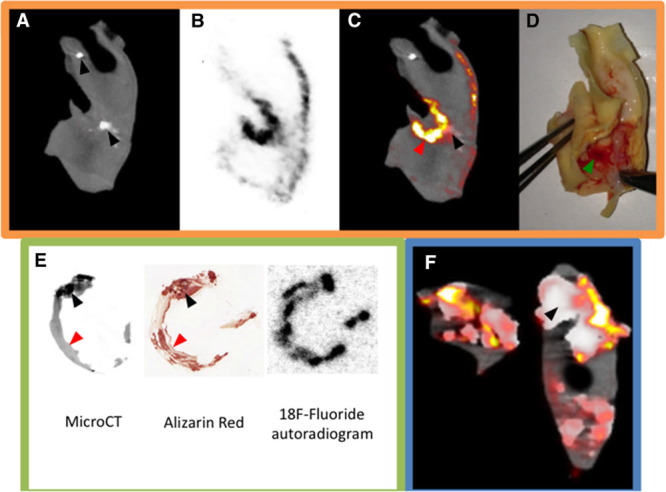
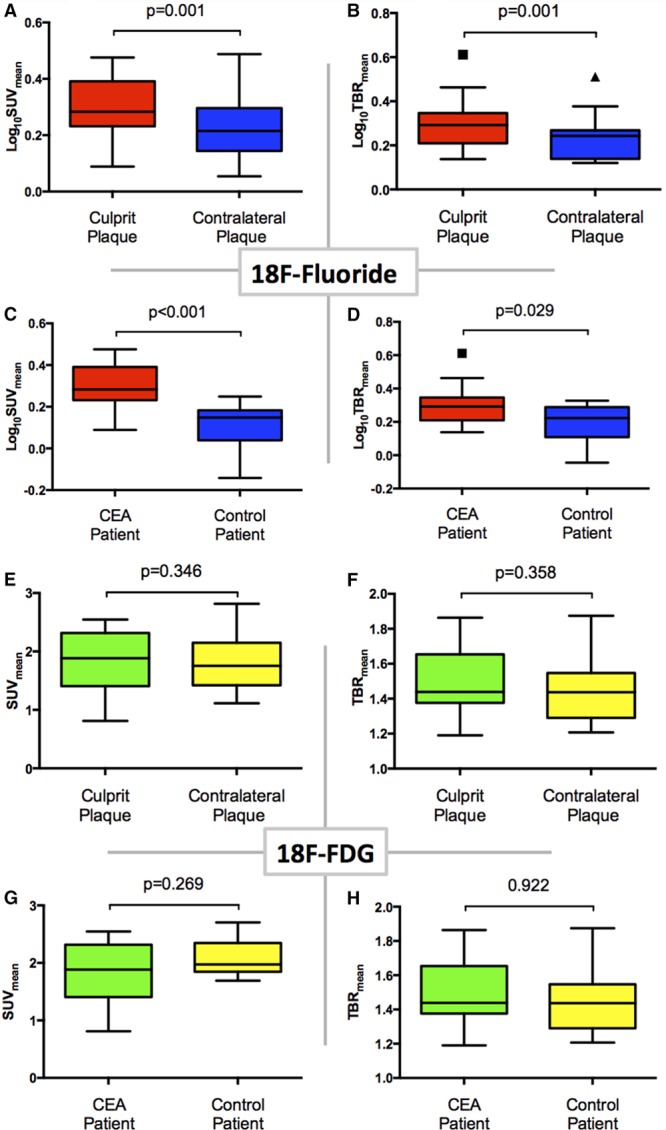
Methods and results: We performed 18F-fluoride and 18F-fluorodeoxyglucose PET/CT in 26 patients after recent transient ischemic attack or minor ischemic stroke: 18 patients with culprit carotid stenosis awaiting carotid endarterectomy and 8 controls without culprit carotid atheroma. We compared standardized uptake values in the clinically adjudicated culprit to the contralateral asymptomatic artery, and assessed the relationship between radiotracer uptake and plaque phenotype or predicted cardiovascular risk (ASSIGN score [Assessing Cardiovascular Risk Using SIGN Guidelines to Assign Preventive Treatment]). We also performed micro PET/CT and histological analysis of excised plaque. On histological and micro PET/CT analysis, 18F-fluoride selectively highlighted microcalcification. Carotid 18F-fluoride uptake was increased in clinically adjudicated culprit plaques compared with asymptomatic contralateral plaques (log10standardized uptake valuemean 0.29±0.10 versus 0.23±0.11, P=0.001) and compared with control patients (log10standardized uptake valuemean 0.29±0.10 versus 0.12±0.11, P=0.001). 18F-Fluoride uptake correlated with high-risk plaque features (remodeling index [r=0.53, P=0.003], plaque burden [r=0.51, P=0.004]), and predicted cardiovascular risk [r=0.65, P=0.002]). Carotid 18F-fluorodeoxyglucose uptake appeared to be increased in 7 of 16 culprit plaques, but no overall differences in uptake were observed in culprit versus contralateral plaques or control patients. However, 18F-fluorodeoxyglucose did correlate with predicted cardiovascular risk (r=0.53, P=0.019), but not with plaque phenotype.
Conclusions: 18F-Fluoride PET/CT highlights culprit and phenotypically high-risk carotid plaque. This has the potential to improve risk stratification and selection of patients who may benefit from intervention.
Keywords: carotid stenosis; fluorides; inflammation; nuclear medicine; phenotype; stroke.
© 2017 The Authors.
Figures

Comment in
-
Molecular Imaging of Atheroma: Deciphering How and When to Use 18F-Sodium Fluoride and 18F-Fluorodeoxyglucose.Circ Cardiovasc Imaging. 2017 Mar;10(3):e006183. doi: 10.1161/CIRCIMAGING.117.006183. Circ Cardiovasc Imaging. 2017. PMID: 28292862 Free PMC article. No abstract available.
References
-
- Rothwell PM, Eliasziw M, Gutnikov SA, Fox AJ, Taylor DW, Mayberg MR, Warlow CP, Barnett HJ Carotid Endarterectomy Trialists’ Collaboration. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361:107–116. - PubMed
-
- Rerkasem K, Rothwell PM. Carotid endarterectomy for symptomatic carotid stenosis. Cochrane Database Syst Rev. 2011:CD001081. - PubMed
-
- Stone GW, Maehara A, Lansky AJ, de Bruyne B, Cristea E, Mintz GS, Mehran R, McPherson J, Farhat N, Marso SP, Parise H, Templin B, White R, Zhang Z, Serruys PW PROSPECT Investigators. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011;364:226–235. doi: 10.1056/NEJMoa1002358. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
