

Curved Walking Rehabilitation with a Rotating Treadmill in Patients with Parkinson's Disease: A Proof of Concept
- PMID: 28293213
- PMCID: PMC5329030
- DOI: 10.3389/fneur.2017.00053
Curved Walking Rehabilitation with a Rotating Treadmill in Patients with Parkinson's Disease: A Proof of Concept
Abstract
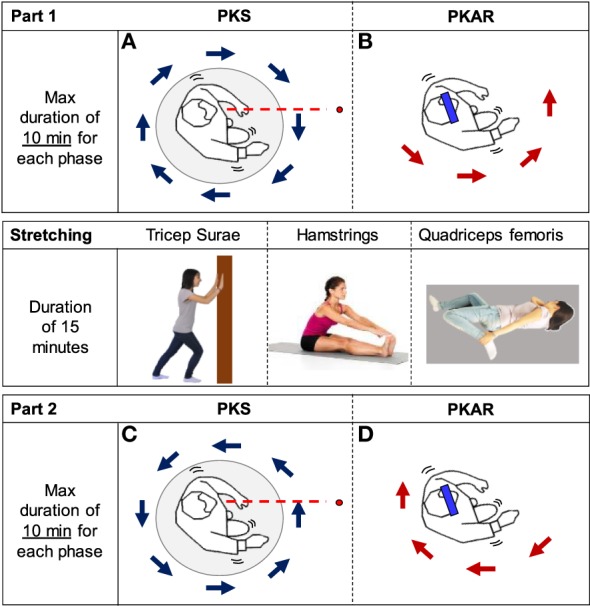
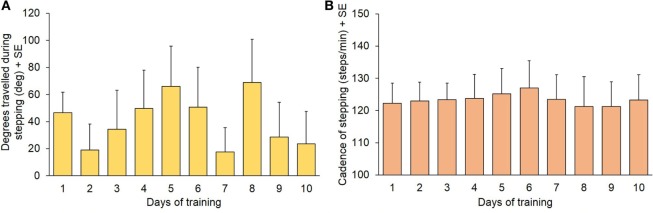
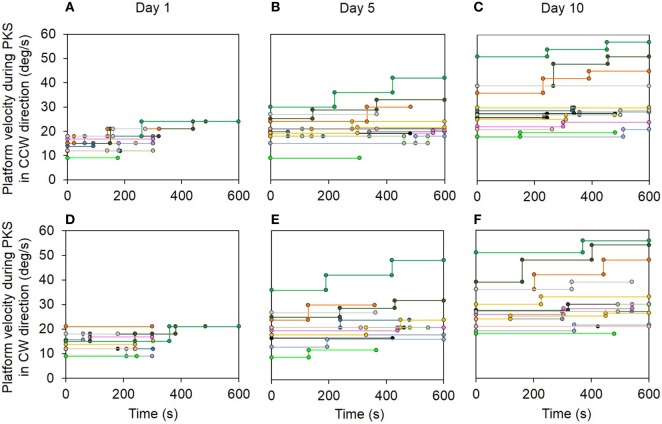
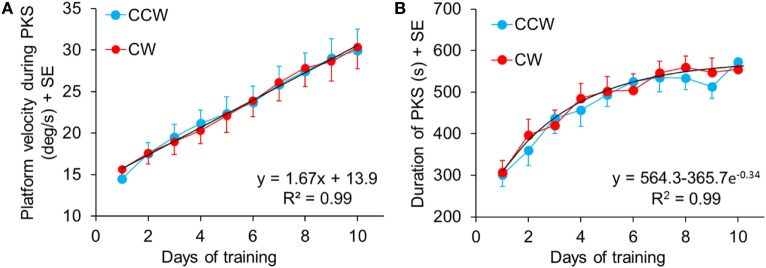
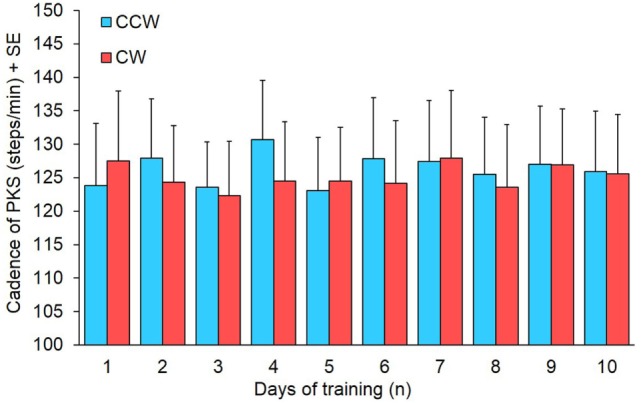
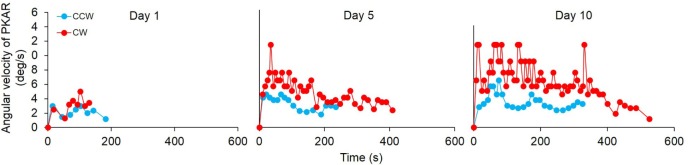
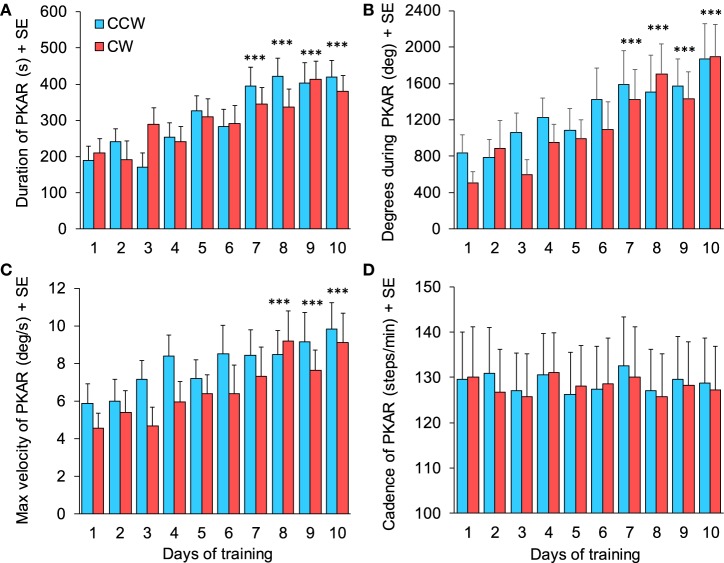
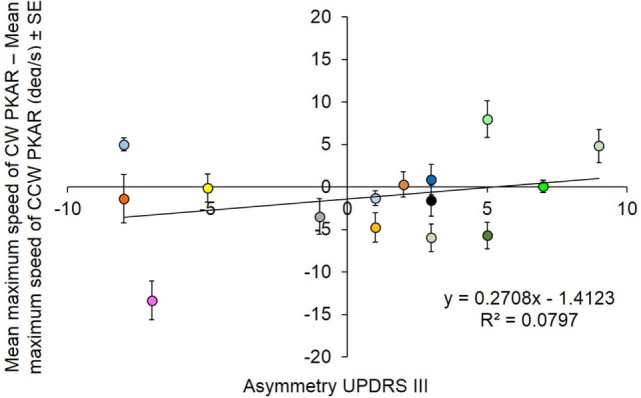
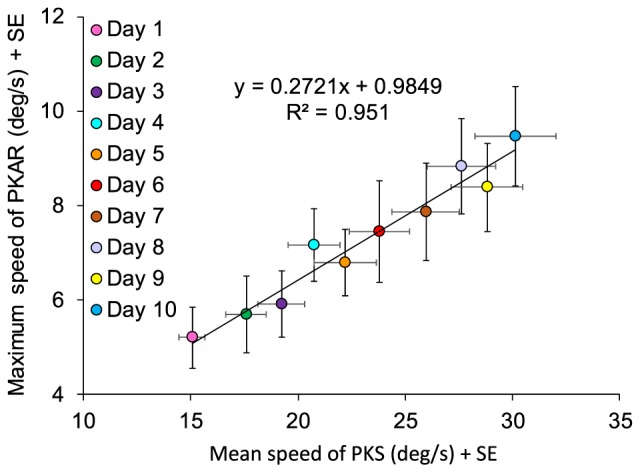
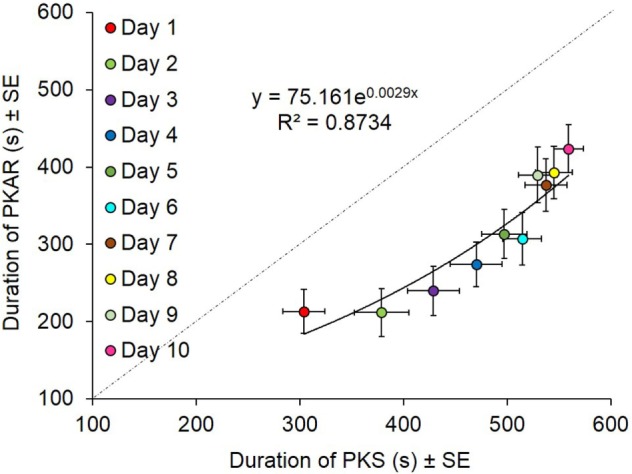
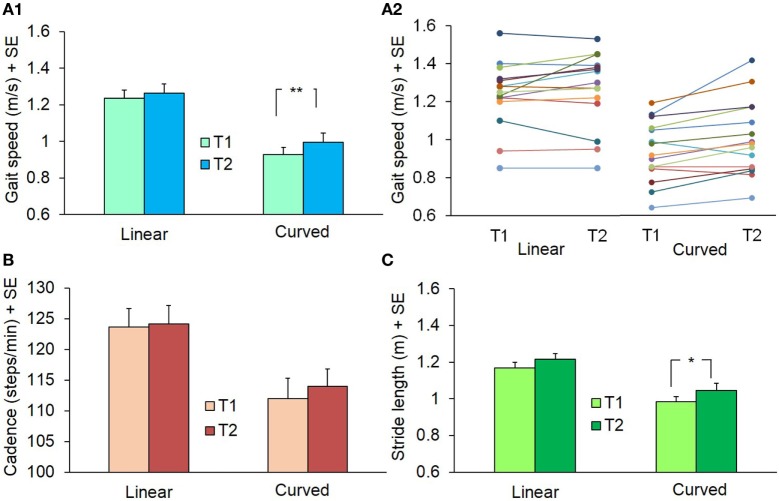
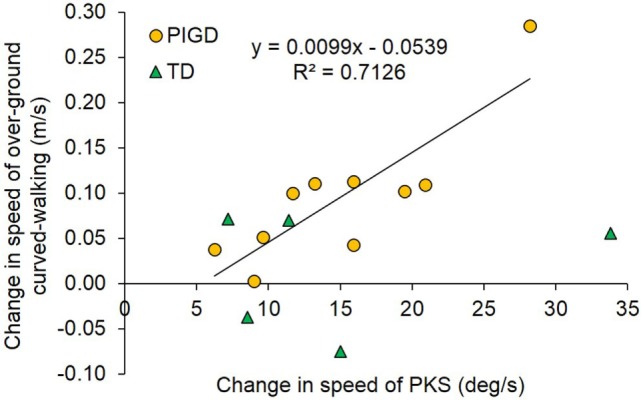
Training subjects to step-in-place eyes open on a rotating platform while maintaining a fixed body orientation in space [podokinetic stimulation (PKS)] produces a posteffect consisting in inadvertent turning around while stepping-in-place eyes closed [podokinetic after-rotation (PKAR)]. Since the rationale for rehabilitation of curved walking in Parkinson's disease is not fully known, we tested the hypothesis that repeated PKS favors the production of curved walking in these patients, who are uneasy with turning, even when straight walking is little affected. Fifteen patients participated in 10 training sessions distributed in 3 weeks. Both counterclockwise and clockwise PKS were randomly administered in each session. PKS velocity and duration were gradually increased over sessions. The velocity and duration of the following PKAR were assessed. All patients showed PKAR, which increased progressively in peak velocity and duration. In addition, before and at the end of the treatment, all patients walked overground along linear and circular trajectories. Post-training, the velocity of walking bouts increased, more so for the circular than the linear trajectory. Cadence was not affected. This study has shown that parkinsonian patients learn to produce turning while stepping when faced with appropriate training and that this capacity translates into improved overground curved walking.
Keywords: Parkinson’s disease; circular treadmill; curved walking; gait rehabilitation; podokinetic after-rotation.
Figures
Similar articles
-
Walking Along Curved Trajectories. Changes With Age and Parkinson's Disease. Hints to Rehabilitation.Front Neurol. 2019 May 24;10:532. doi: 10.3389/fneur.2019.00532. eCollection 2019. Front Neurol. 2019. PMID: 31178816 Free PMC article. Review.
-
Podokinetic After-Rotation Is Transiently Enhanced or Reversed by Unilateral Axial Muscle Proprioceptive Stimulation.Neural Plast. 2019 Mar 11;2019:7129279. doi: 10.1155/2019/7129279. eCollection 2019. Neural Plast. 2019. PMID: 30984256 Free PMC article.
-
Stepping in Place While Voluntarily Turning Around Produces a Long-Lasting Posteffect Consisting in Inadvertent Turning While Stepping Eyes Closed.Neural Plast. 2016;2016:7123609. doi: 10.1155/2016/7123609. Epub 2016 Aug 22. Neural Plast. 2016. PMID: 27635264 Free PMC article.
-
Transfer of podokinetic adaptation from stepping to hopping.J Neurophysiol. 2002 Feb;87(2):1142-4. doi: 10.1152/jn.00588.2001. J Neurophysiol. 2002. PMID: 11826080
-
Turning problems and freezing of gait in Parkinson's disease: a systematic review and meta-analysis.Disabil Rehabil. 2019 Dec;41(25):2994-3004. doi: 10.1080/09638288.2018.1483429. Epub 2018 Jun 30. Disabil Rehabil. 2019. PMID: 29961369
Cited by
-
Walking Along Curved Trajectories. Changes With Age and Parkinson's Disease. Hints to Rehabilitation.Front Neurol. 2019 May 24;10:532. doi: 10.3389/fneur.2019.00532. eCollection 2019. Front Neurol. 2019. PMID: 31178816 Free PMC article. Review.
-
Podokinetic After-Rotation Is Transiently Enhanced or Reversed by Unilateral Axial Muscle Proprioceptive Stimulation.Neural Plast. 2019 Mar 11;2019:7129279. doi: 10.1155/2019/7129279. eCollection 2019. Neural Plast. 2019. PMID: 30984256 Free PMC article.
-
The Effect of Different Turn Speeds on Whole-Body Coordination in Younger and Older Healthy Adults.Sensors (Basel). 2021 Apr 16;21(8):2827. doi: 10.3390/s21082827. Sensors (Basel). 2021. PMID: 33923838 Free PMC article.
-
Basic Spatiotemporal Gait Variables of Young and Older Healthy Volunteers Walking Along a Novel Figure-of-8 Path.Front Neurol. 2021 Jun 8;12:698160. doi: 10.3389/fneur.2021.698160. eCollection 2021. Front Neurol. 2021. PMID: 34168613 Free PMC article.
References
-
- Morris ME, Huxham FE, McGinley J, Iansek R. Gait disorders and gait rehabilitation in Parkinson’s disease. Adv Neurol (2001) 87:347–61. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous