

Vertically Set Sombrero-shaped Abdominal Flap for Asian Breast Reconstruction after Skin-sparing Mastectomy
- PMID: 28293497
- PMCID: PMC5222642
- DOI: 10.1097/GOX.0000000000001123
Vertically Set Sombrero-shaped Abdominal Flap for Asian Breast Reconstruction after Skin-sparing Mastectomy
Abstract
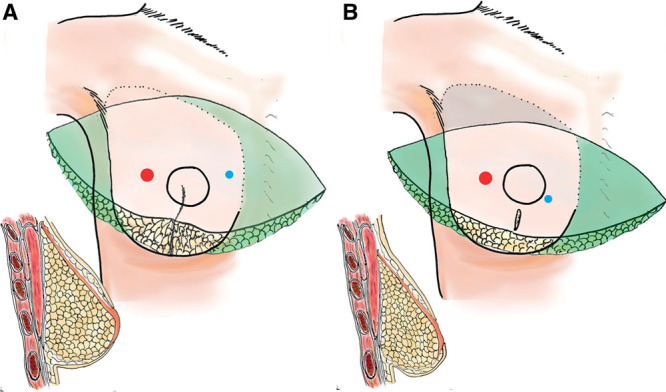
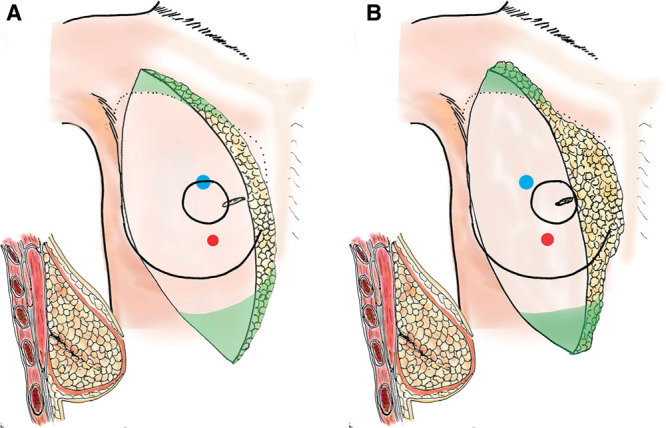
Background: Immediate autologous breast reconstruction after skin-sparing mastectomy is an esthetically superior method, and a free abdominal flap is often used. However, in Asian patients, little redundant abdominal skin and thin subcutaneous tissue are common, necessitating the development of a more suitable flap design and setting. We devised a narrow flap, the sombrero-shaped flap (S-flap), set vertically, to reduce postoperative abdominal morbidity without sacrificing cosmetic results.
Methods: To assess this new flap design and setting, the recipient- and donor-site complications of consecutive patients treated by S-flap (n = 40) and conventional flap (C-flap) (n = 22) were retrospectively investigated. Postoperative abdominal pain, stiffness, and patient activity were also assessed in each group with our original grading scale.
Results: Compared with the C-flap group, the S-flap group had a significantly lower skin paddle vertical height (mean, 14.0 and 10.2 cm, respectively; P < 0.001), lower abdominal stiffness (P = 0.023), and higher rate of double-pedicled flap use (27.3% and 52.5%, respectively; P < 0.048). The rates of donor and recipient site complications, postoperative abdominal pain, and activity did not significantly differ between the groups.
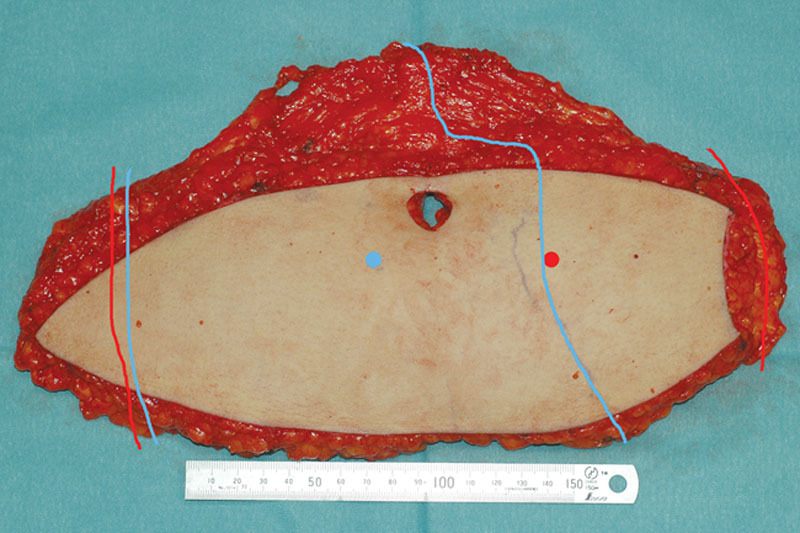
Conclusions: For immediate breast reconstruction after skin-sparing mastectomy in Asian patients, our newly designed S-flap and vertical flap setting achieved cosmetically good, consistent results with low abdominal morbidity, even though the abdominal flap was thin and narrow. The viability of the S-flap, including medial fan-shaped adipose flap, was reliable, even though the flap often required elevation with double pedicles.
Figures
Similar articles
-
Immediate breast reconstruction with the transverse rectus abdominis musculocutaneous flap after skin-sparing mastectomy.Int Surg. 2001 Oct-Dec;86(4):246-51. Int Surg. 2001. PMID: 12056470
-
Immediate breast reconstruction with expander assisted latissimus dorsi flap after skin sparing mastectomy.J Egypt Natl Canc Inst. 2006 Jun;18(2):134-40. J Egypt Natl Canc Inst. 2006. PMID: 17496938
-
The transverse myocutaneous gracilis free flap: a valuable tissue source in autologous breast reconstruction.Plast Reconstr Surg. 2004 Jul;114(1):69-73. doi: 10.1097/01.prs.0000127797.62020.d4. Plast Reconstr Surg. 2004. PMID: 15220571
-
Donor site selection and clinical outcomes of nipple-areola skin-sparing mastectomy with immediate autologous free flap reconstruction: A single-institution experience.Eur J Surg Oncol. 2016 Mar;42(3):369-75. doi: 10.1016/j.ejso.2015.12.002. Epub 2015 Dec 29. Eur J Surg Oncol. 2016. PMID: 26792708
-
Optimizing pedicled transverse rectus abdominis muscle flap breast reconstruction.Cancer J. 2008 Jul-Aug;14(4):236-40. doi: 10.1097/PPO.0b013e318180bce5. Cancer J. 2008. PMID: 18677131 Review.
Cited by
-
Abdominal-Based Microsurgical Breast Reconstruction: How to Inset the Flap to Maximize the Aesthetic Result-A Systematic Review.J Clin Med. 2023 Sep 22;12(19):6135. doi: 10.3390/jcm12196135. J Clin Med. 2023. PMID: 37834779 Free PMC article. Review.
-
Techniques of inserting deep inferior epigastric perforator flap obliquely in immediate breast reconstruction after total mastectomy.JPRAS Open. 2023 Jan 24;36:1-7. doi: 10.1016/j.jpra.2023.01.001. eCollection 2023 Jun. JPRAS Open. 2023. PMID: 36844476 Free PMC article.
-
Shaping of the abdominal flap in breast reconstruction: The coning technique in muscle sparing TRAM.JPRAS Open. 2020 Jul 31;25:93-98. doi: 10.1016/j.jpra.2020.07.003. eCollection 2020 Sep. JPRAS Open. 2020. PMID: 32904163 Free PMC article.
References
-
- Carlson GW. Skin sparing mastectomy: anatomic and technical considerations. Am Surg. 1996;62:151–155. - PubMed
-
- Hidalgo DA. Aesthetic refinement in breast reconstruction: complete skin-sparing mastectomy with autogenous tissue transfer. Plast Reconstr Surg. 1998;102:63–70. discussion 71. - PubMed
-
- Slavin SA, Schnitt SJ, Duda RB, et al. Skin-sparing mastectomy and immediate reconstruction: oncologic risks and aesthetic results in patients with early-stage breast cancer. Plast Reconstr Surg. 1998;102:49–62. - PubMed
-
- Foster RD, Esserman LJ, Anthony JP, et al. Skin-sparing mastectomy and immediate breast reconstruction: a prospective cohort study for the treatment of advanced stages of breast carcinoma. Ann Surg Oncol. 2002;9:462–466. - PubMed
-
- Patani N, Mokbel K. Oncological and aesthetic considerations of skin-sparing mastectomy. Breast Cancer Res Treat. 2008;111:391–403. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources