

Thyroglossal Duct Cyst Carcinomas in Pediatric Patients: Report of Two Cases with a Comprehensive Literature Review
- PMID: 28293858
- PMCID: PMC5677077
- DOI: 10.1007/s12105-017-0807-0
Thyroglossal Duct Cyst Carcinomas in Pediatric Patients: Report of Two Cases with a Comprehensive Literature Review
Abstract
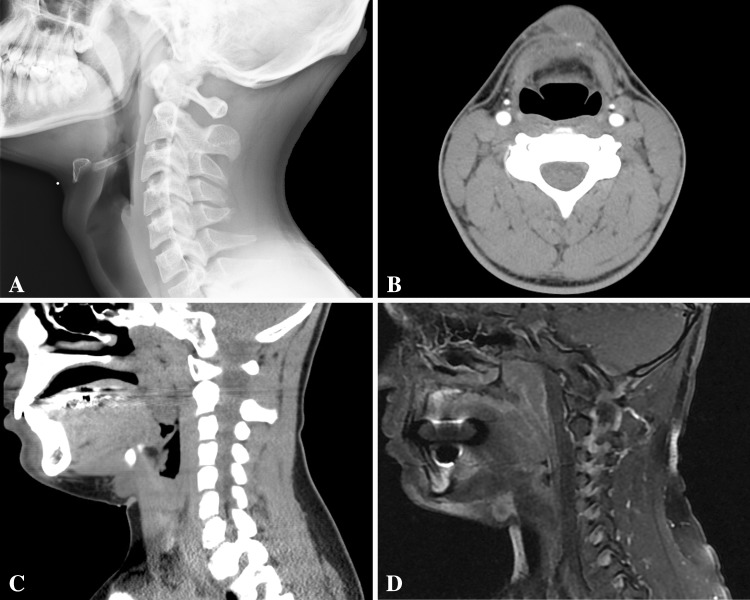
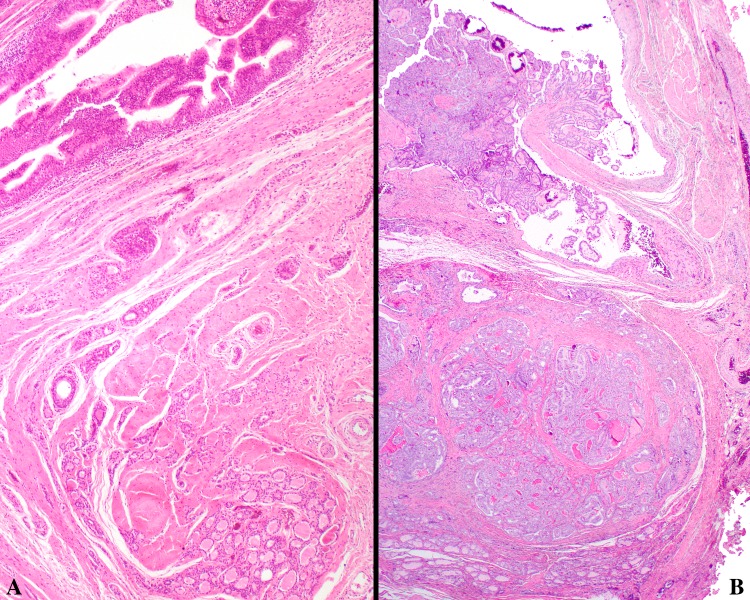
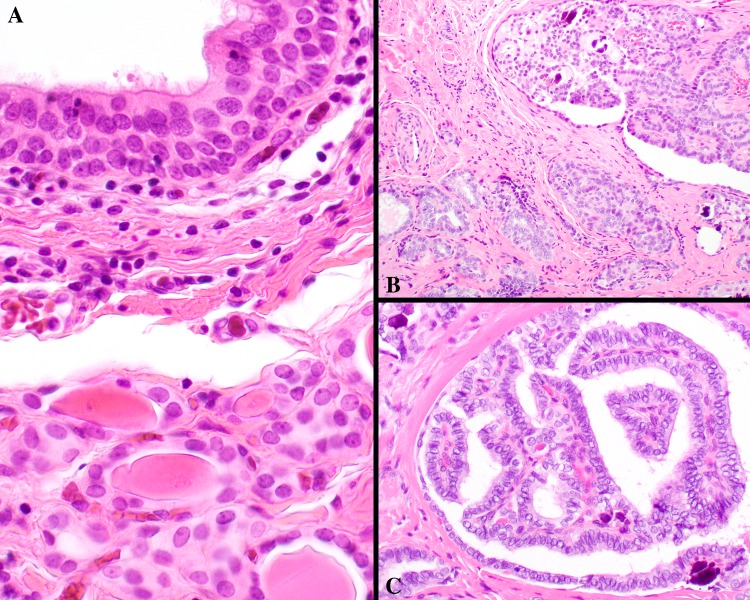
Thyroglossal duct cyst (TGDC) carcinomas are rarely encountered in the pediatric population. The clinical behavior of these tumors in the pediatric setting is unclear and management is not well defined. Two cases of pediatric thyroglossal duct cyst carcinoma were identified in a review of all thyroglossal duct cysts diagnosed over a ten year period. These two cases were analyzed along with 57 cases of thyroglossal duct cyst carcinoma affecting patients less than 21 years of age compiled from the English literature. Fifty-nine patients (36 females, 23 males) aged 6-20 years (mean 15.0 years) were identified. All presented with an anterior midline neck mass, which was typically mobile and non-tender. The average tumor size was 2.6 cm. Histologically, all tumors were papillary thyroid carcinomas arising in a background of a thyroglossal duct cyst. The tumors exhibited a papillary, follicular, or mixed architecture with classical papillary thyroid carcinoma nuclear features. Soft tissue extension was present in 16 cases. All patients were managed surgically with a Sistrunk procedure, with additional thyroidectomy performed in 29 patients, combined with a lymph node dissection (n = 15), or a Sistrunk and lymph node dissection (n = 5). All patients were stage I at presentation, with 11 showing lymph node metastases. Postoperative radioactive iodine was employed in 20 patients. A papillary carcinoma of the thyroid gland was reported in four of the patients who had concurrent/subsequent thyroidectomies. Recurrences were reported in four patients, with distant metastases in one patient, who died of disease (13 months). Follow up data was available for 45 patients, with an overall mean follow-up of 54.5 months. All patients were alive, with the exception of one who died with disease. TGDC carcinomas in pediatric patients is associated with a good overall prognosis, best managed by Sistrunk procedure alone, with selected lymph node dissection if clinically indicated.
Keywords: Adolescence; Carcinoma, papillary; Childhood; Follow-up studies; Incidence; Pediatric; Prognosis; Thyroglossal duct cyst; Thyroid neoplasms; Thyroidectomy.
Conflict of interest statement
Conflict of interest
All authors declare there are no conflicts of interest. The opinions or assertions contained herein are the private views of the author and are not to be construed as official or as reflecting the views of Southern California Permanente Medical Group.
Ethical Approval
All research was retrospective involving human participants in accordance with the ethical standards of the institution with IRB approval #5968.
Figures
References
-
- Allard RH. The thyroglossal cyst. Head Neck Surg. 1982;5(2):134–146. - PubMed
-
- Chou J, Walters A, Hage R, Zurada A, Michalak M, Tubbs RS, et al. Thyroglossal duct cysts: anatomy, embryology and treatment. Surg Radiol Anat. 2013;35(10):875–881. - PubMed
-
- Baltar BJ, Pineiro MH, Estevez DA, Campo Blanco MC, Ferrandez RM, Gil GP. [Differentiated thyroid cancer on the thyroglossal duct] J Chir. 1991;128(10):441–445. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
