

How Can Genetic Studies Help Us to Understand Links Between Birth Weight and Type 2 Diabetes?
- PMID: 28293907
- PMCID: PMC5350261
- DOI: 10.1007/s11892-017-0852-9
How Can Genetic Studies Help Us to Understand Links Between Birth Weight and Type 2 Diabetes?
Abstract
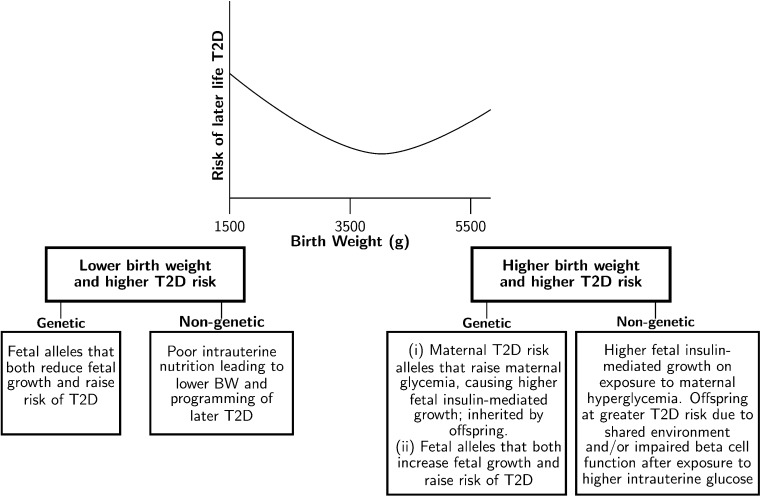
Purpose of review: In observational epidemiology, both low and high birth weights are associated with later type 2 diabetes. The mechanisms underlying the associations are poorly understood. We review evidence for the roles of genetic and non-genetic factors linking both sides of the birth weight distribution to risk of type 2 diabetes, focusing on contributions made by the most recent genome-wide association studies (GWAS) of birth weight.
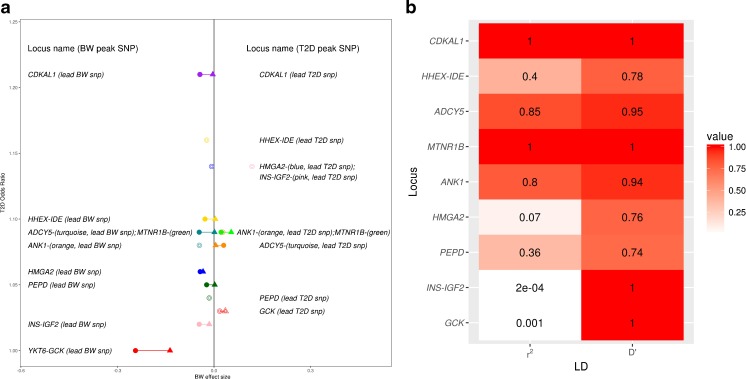
Recent findings: There are now nine genetic loci robustly implicated in both fetal growth and type 2 diabetes. At many of these, the same alleles are associated both with a higher risk of type 2 diabetes and a lower birth weight. This supports the Fetal Insulin Hypothesis and reflects a general pattern for type 2 diabetes susceptibility alleles: genome-wide, there is an inverse genetic correlation with birth weight, and initial estimates suggest genetic factors explain a large part of the covariance between the two traits. However, the associations at individual loci show heterogeneity; some fetal risk alleles are associated with higher birth weight. For most of these, the association reflects their correlation with the maternal risk allele which raises maternal glucose, thus increasing fetal insulin-mediated growth. GWAS have improved our understanding of the mechanisms underlying associations between type 2 diabetes and birth weight but questions remain about the relative importance of genetic versus non-genetic factors and of maternal versus fetal genotypes. To answer these questions, future work will require well-powered analyses of parents and offspring.
Keywords: Birth weight; Fetal; Genetics; Genome-wide association study; Maternal; Type 2 diabetes.
Conflict of interest statement
Conflict of Interest
Dr. Beaumont and Dr. Freathy report grant funding from Wellcome Trust and Royal Society. Dr. Horikoshi has nothing to disclose.
Prof. McCarthy reports grants and personal fees from Novo Nordisk, Eli Lilly, and Pfizer, and grants from Takeda, Roche, Sanofi Aventis, Boehringer Ingelheim, Servier, Janssens, Abbvie, and Astra Zeneca.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
