

Rationale and design of REDUCE-IT: Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial
- PMID: 28294373
- PMCID: PMC5396348
- DOI: 10.1002/clc.22692
Rationale and design of REDUCE-IT: Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial
Abstract
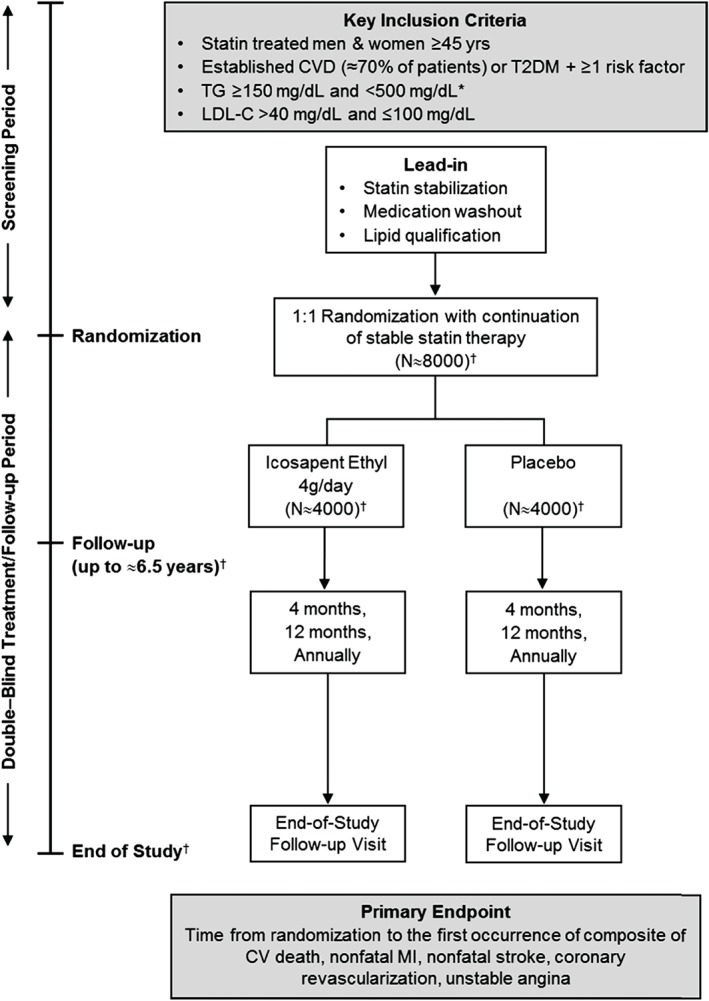
Residual cardiovascular risk persists despite statins, yet outcome studies of lipid-targeted therapies beyond low-density lipoprotein cholesterol (LDL-C) have not demonstrated added benefit. Triglyceride elevation is an independent risk factor for cardiovascular events. High-dose eicosapentaenoic acid (EPA) reduces triglyceride-rich lipoproteins without raising LDL-C. Omega-3s have postulated pleiotropic cardioprotective benefits beyond triglyceride-lowering. To date, no large, multinational, randomized clinical trial has proved that lowering triglycerides on top of statin therapy improves cardiovascular outcomes. The Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial (REDUCE-IT; NCT01492361) is a phase 3b randomized, double-blinded, placebo-controlled trial of icosapent ethyl, a highly purified ethyl ester of EPA, vs placebo. The main objective is to evaluate whether treatment with icosapent ethyl reduces ischemic events in statin-treated patients with high triglycerides at elevated cardiovascular risk. REDUCE-IT enrolled men or women age ≥45 years with established cardiovascular disease or age ≥50 years with diabetes mellitus and 1 additional risk factor. Randomization required fasting triglycerides ≥150 mg/dL and <500 mg/dL and LDL-C >40 mg/dL and ≤100 mg/dL with stable statin (± ezetimibe) ≥4 weeks prior to qualifying measurements. The primary endpoint is a composite of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, coronary revascularization, or unstable angina. The key secondary endpoint is the composite of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke. Several secondary, tertiary, and exploratory endpoints will be assessed. Approximately 8000 patients have been randomized at approximately 470 centers worldwide. Follow-up will continue in this event-driven trial until approximately 1612 adjudicated primary-efficacy endpoint events have occurred.
Keywords: Clinical trials; General clinical cardiology/adult; Lipidology.
© 2017 The Authors. Clinical Cardiology published by Wiley Periodicals, Inc.
Conflict of interest statement
Dr. Bhatt has served on advisory boards for Cardax, Elsevier Practice Update Cardiology, Medscape Cardiology, and Regado Biosciences; has served on the board of directors for Boston VA Research Institute and Society of Cardiovascular Patient Care; has been chair of the American Heart Association Quality Oversight Committee; has served on data monitoring committees for Duke Clinical Research Institute, Harvard Clinical Research Institute, Mayo Clinic, and the Population Health Research Institute; has received honoraria from the American College of Cardiology (senior associate editor, clinical trials and news, for
Figures
References
-
- Klempfner R, Erez A, Sagit BZ, et al. Elevated triglyceride level is independently associated with increased all‐cause mortality in patients with established coronary heart disease: twenty‐two‐year follow‐up of the Bezafibrate Infarction Prevention Study and Registry [published correction appears in Circ Cardiovasc Qual Outcomes. 2016;9:613]. Circ Cardiovasc Qual Outcomes . 2016;9:100–108. - PubMed
-
- Nordestgaard BG. Triglyceride‐rich lipoproteins and atherosclerotic cardiovascular disease: new insights from epidemiology, genetics, and biology. Circ Res. 2016;118:547–563. - PubMed
-
- Saito Y, Yokoyama M, Origasa H, et al; JELIS Investigators . Effects of EPA on coronary artery disease in hypercholesterolemic patients with multiple risk factors: sub‐analysis of primary prevention cases from the Japan EPA Lipid Intervention Study (JELIS) [published correction appears in Atherosclerosis. 2009;204:233]. Atherosclerosis . 2008;200:135–140. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
