

Hospital Readmission and Social Risk Factors Identified from Physician Notes
- PMID: 28295260
- PMCID: PMC5867172
- DOI: 10.1111/1475-6773.12670
Hospital Readmission and Social Risk Factors Identified from Physician Notes
Abstract
Objective: To evaluate the prevalence of seven social factors using physician notes as compared to claims and structured electronic health records (EHRs) data and the resulting association with 30-day readmissions.
Study setting: A multihospital academic health system in southeastern Massachusetts.
Study design: An observational study of 49,319 patients with cardiovascular disease admitted from January 1, 2011, to December 31, 2013, using multivariable logistic regression to adjust for patient characteristics.
Data collection/extraction methods: All-payer claims, EHR data, and physician notes extracted from a centralized clinical registry.
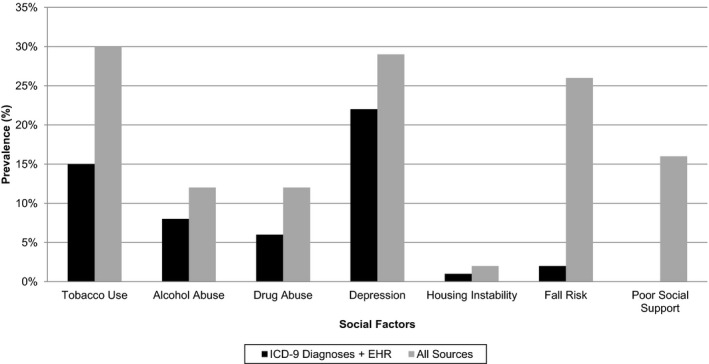
Principal findings: All seven social characteristics were identified at the highest rates in physician notes. For example, we identified 14,872 patient admissions with poor social support in physician notes, increasing the prevalence from 0.4 percent using ICD-9 codes and structured EHR data to 16.0 percent. Compared to an 18.6 percent baseline readmission rate, risk-adjusted analysis showed higher readmission risk for patients with housing instability (readmission rate 24.5 percent; p < .001), depression (20.6 percent; p < .001), drug abuse (20.2 percent; p = .01), and poor social support (20.0 percent; p = .01).
Conclusions: The seven social risk factors studied are substantially more prevalent than represented in administrative data. Automated methods for analyzing physician notes may enable better identification of patients with social needs.
Keywords: Social determinants of health; natural language processing; quality of care; readmissions.
© Health Research and Educational Trust.
Figures
- 1
Notes: The black bars indicate the prevalence in the sample for each social factor in
ICD ‐9 codes plus structuredEHR , and the gray bars indicate the prevalence when using all sources including physician notes.
References
-
- Akosah, K. O. , Schaper A. M., Haus L. M., Mathiason M. A., Barnhart S. I., and McHugh V. L.. 2005. “Improving Outcomes in Heart Failure in the Community: Long‐Term Survival Benefit of a Disease‐Management Program.” Chest 127 (6): 2042–8. - PubMed
-
- Allaudeen, N. , Vidyarthi A., Maselli J., and Auerbach A.. 2011. “Redefining Readmission Risk Factors for General Medicine Patients.” Journal of Hospital Medicine 6 (2): 54–60. - PubMed
-
- Amarasingham, R. , Moore B. J., Tabak Y. P., Drazner M. H., Clark C. A., Zhang S., Reed W. G., Swanson T. S., Ma Y., and Halm E. A.. 2010. “An Automated Model to Identify Heart Failure Patients at Risk for 30‐Day Readmission or Death Using Electronic Medical Record Data.” Medical Care 48 (11): 981–8. - PubMed
-
- Anchersen, K. , Clausen T., Gossop M., Hansteen V., and Waal H.. 2009. “Prevalence and Clinical Relevance of Corrected QT Interval Prolongation during Methadone and Buprenorphine Treatment: A Mortality Assessment Study.” Addiction 104 (6): 993–9. - PubMed
-
- Arbaje, A. I. , Wolff J. L., Yu Q., Powe N. R., Anderson G. F., and Boult C.. 2008. “Postdischarge Environmental and Socioeconomic Factors and the Likelihood of Early Hospital Readmission among Community‐Dwelling Medicare Beneficiaries.” Gerontologist 48 (4): 495–504. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
