

Young adult outcomes in the follow-up of the multimodal treatment study of attention-deficit/hyperactivity disorder: symptom persistence, source discrepancy, and height suppression
- PMID: 28295312
- PMCID: PMC6168061
- DOI: 10.1111/jcpp.12684
Young adult outcomes in the follow-up of the multimodal treatment study of attention-deficit/hyperactivity disorder: symptom persistence, source discrepancy, and height suppression
Abstract
Background: The Multimodal Treatment Study (MTA) began as a 14-month randomized clinical trial of behavioral and pharmacological treatments of 579 children (7-10 years of age) diagnosed with attention-deficit/hyperactivity disorder (ADHD)-combined type. It transitioned into an observational long-term follow-up of 515 cases consented for continuation and 289 classmates (258 without ADHD) added as a local normative comparison group (LNCG), with assessments 2-16 years after baseline.
Methods: Primary (symptom severity) and secondary (adult height) outcomes in adulthood were specified. Treatment was monitored to age 18, and naturalistic subgroups were formed based on three patterns of long-term use of stimulant medication (Consistent, Inconsistent, and Negligible). For the follow-up, hypothesis-generating analyses were performed on outcomes in early adulthood (at 25 years of age). Planned comparisons were used to estimate ADHD-LNCG differences reflecting persistence of symptoms and naturalistic subgroup differences reflecting benefit (symptom reduction) and cost (height suppression) associated with extended use of medication.
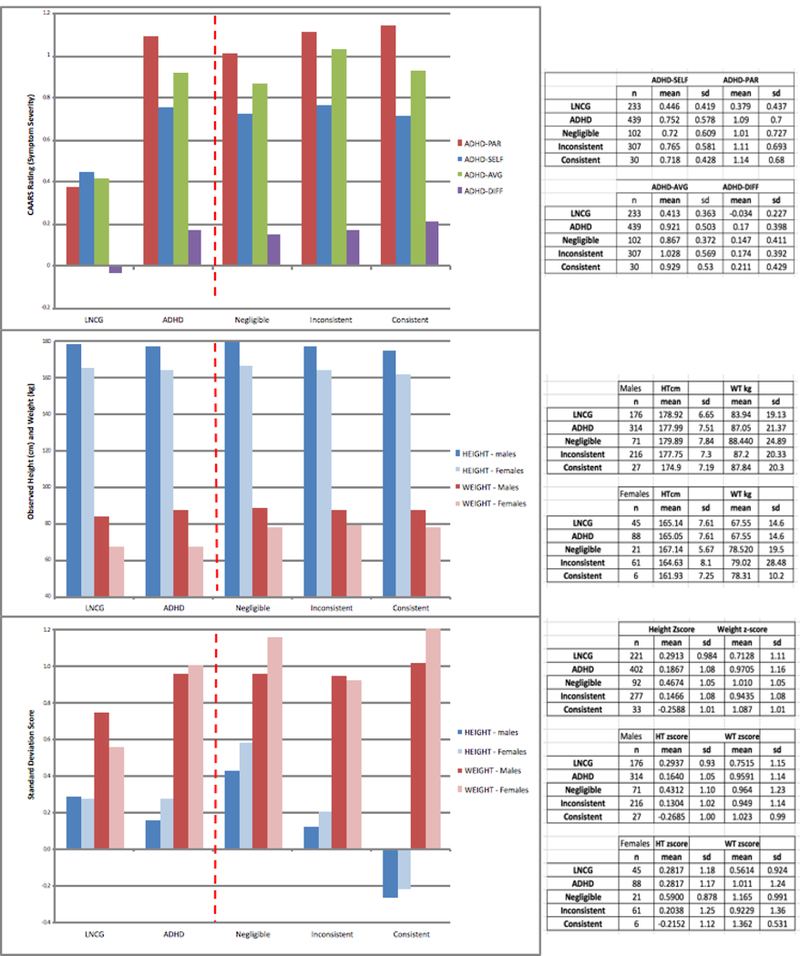
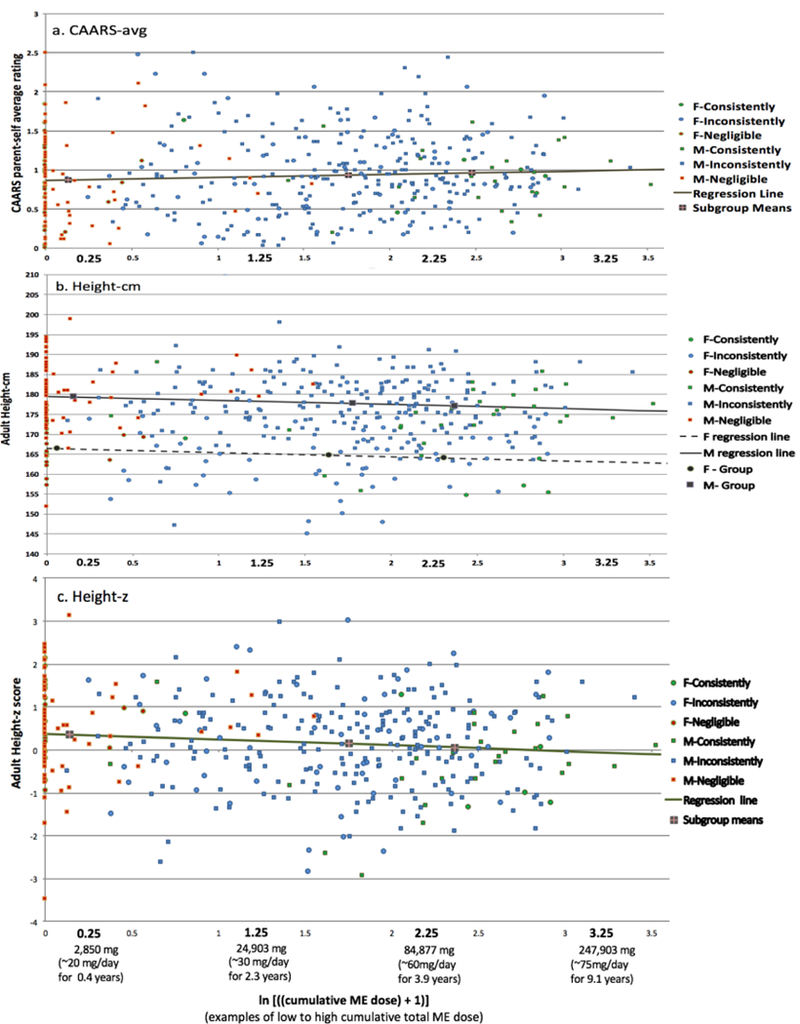
Results: For ratings of symptom severity, the ADHD-LNCG comparison was statistically significant for the parent/self-report average (0.51 ± 0.04, p < .0001, d = 1.11), documenting symptom persistence, and for the parent/self-report difference (0.21 ± 0.04, p < .0001, d = .60), documenting source discrepancy, but the comparisons of naturalistic subgroups reflecting medication effects were not significant. For adult height, the ADHD group was 1.29 ± 0.55 cm shorter than the LNCG (p < .01, d = .21), and the comparisons of the naturalistic subgroups were significant: the treated group with the Consistent or Inconsistent pattern was 2.55 ± 0.73 cm shorter than the subgroup with the Negligible pattern (p < .0005, d = .42), and within the treated group, the subgroup with the Consistent pattern was 2.36 ± 1.13 cm shorter than the subgroup with the Inconsistent pattern (p < .04, d = .38).
Conclusions: In the MTA follow-up into adulthood, the ADHD group showed symptom persistence compared to local norms from the LNCG. Within naturalistic subgroups of ADHD cases, extended use of medication was associated with suppression of adult height but not with reduction of symptom severity.
Keywords: Attention-deficit/hyperactivity disorder; follow-up studies; growth; longitudinal studies; medication effects; treatment trials.
© 2017 Association for Child and Adolescent Mental Health.
Conflict of interest statement
Conflict of interest statement: See Acknowledgements for disclosures.
Figures
References
-
- American Academy of Pediatrics, Subcommittee on Attention-Deficit/Hyperactivity Disorder, Steering Committee on Quality Improvement and Management. Pediatrics. 2011; 128: 1–14.
-
- Barkley R, Murphy K, Fischer M. ADHD in Adults: What Science Says. NY: Guilford; 2008.
-
- Biederman J, Monuteaux MC, Spencer T, et al. Stimulant therapy and risk for subsequent substance use disorders in male adults with ADHD: A naturalistic controlled 10-year follow-up study. Am J Psychiatry. 2008; 165: 597–603. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 MH050467/MH/NIMH NIH HHS/United States
- N01 MH012008/MH/NIMH NIH HHS/United States
- U01 MH050461/MH/NIMH NIH HHS/United States
- HHSN271200800008C/DA/NIDA NIH HHS/United States
- U01 MH050440/MH/NIMH NIH HHS/United States
- N01 DA085550/DA/NIDA NIH HHS/United States
- N01 DA085548/DA/NIDA NIH HHS/United States
- N01 MH012012/MH/NIMH NIH HHS/United States
- HHSN271200800003C/DA/NIDA NIH HHS/United States
- N01 DA085549/DA/NIDA NIH HHS/United States
- N01 MH012010/MH/NIMH NIH HHS/United States
- HHSN271200800009C/DA/NIDA NIH HHS/United States
- HHSN271200800005C/DA/NIDA NIH HHS/United States
- U54 HD090257/HD/NICHD NIH HHS/United States
- HHSN271200800006C/DA/NIDA NIH HHS/United States
- N01 DA085553/DA/NIDA NIH HHS/United States
- N01 MH012011/MH/NIMH NIH HHS/United States
- K23 DA032577/DA/NIDA NIH HHS/United States
- N01 MH012004/MH/NIMH NIH HHS/United States
- N01 DA085554/DA/NIDA NIH HHS/United States
- N01 MH012009/MH/NIMH NIH HHS/United States
- U01 MH050453/MH/NIMH NIH HHS/United States
- N01 MH012007/MH/NIMH NIH HHS/United States
- N01 DA085551/DA/NIDA NIH HHS/United States
- HHSN271200800007C/DA/NIDA NIH HHS/United States
- R01 DA039881/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
