

Preoperative use of pregabalin for acute pain in spine surgery: A meta-analysis of randomized controlled trials
- PMID: 28296725
- PMCID: PMC5369880
- DOI: 10.1097/MD.0000000000006129
Preoperative use of pregabalin for acute pain in spine surgery: A meta-analysis of randomized controlled trials
Abstract
Background: We performed a systematic review and meta-analysis of randomized controlled trials (RCTs) to evaluate the efficacy and safety of pregabalin for pain management following spine surgery.
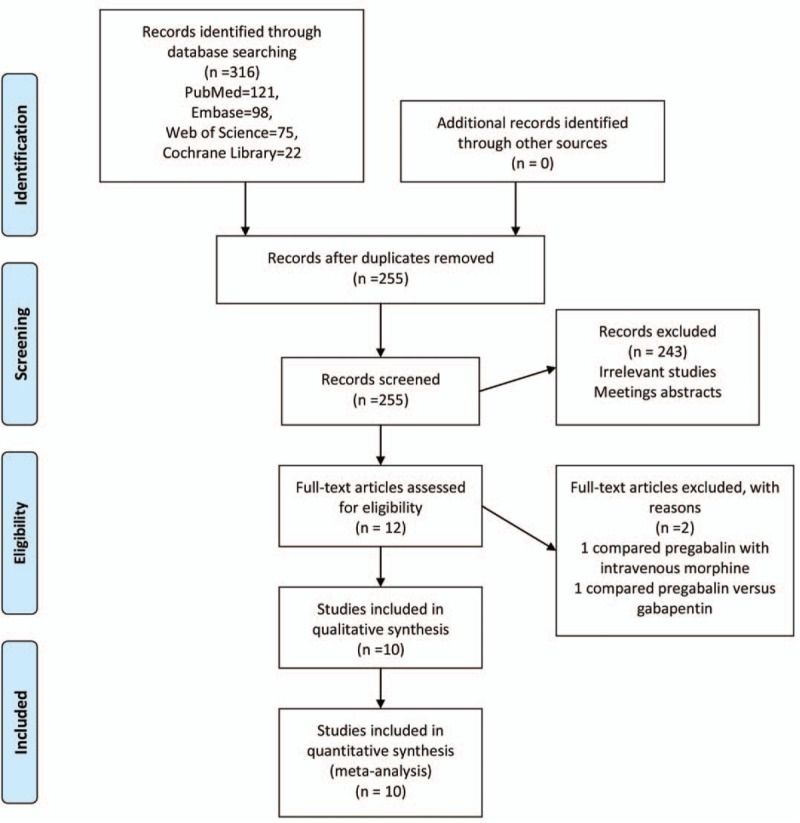
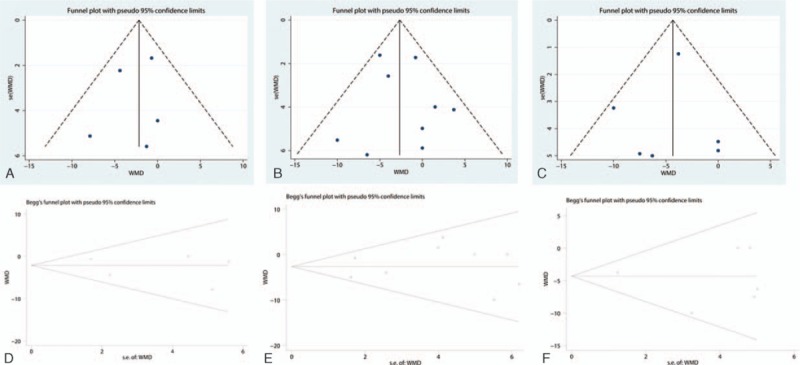
Methods: In September 2016, a systematic computer-based search was conducted in PubMed, EMBASE, Web of Science, and Cochrane Database of Systematic Reviews. RCTs of patients prepared for spine surgery that compared pregabalin with placebo were retrieved. The primary endpoint was the VAS score with rest or mobilization at 12 hours, 24 hours, and 48 hours and cumulative morphine consumption at 24 hours and 48 hours. The secondary outcomes were complications of nausea, sedation, dizziness, headache, and visual disturbances. After testing for publication bias and heterogeneity between studies, data were aggregated for random-effects models when necessary.
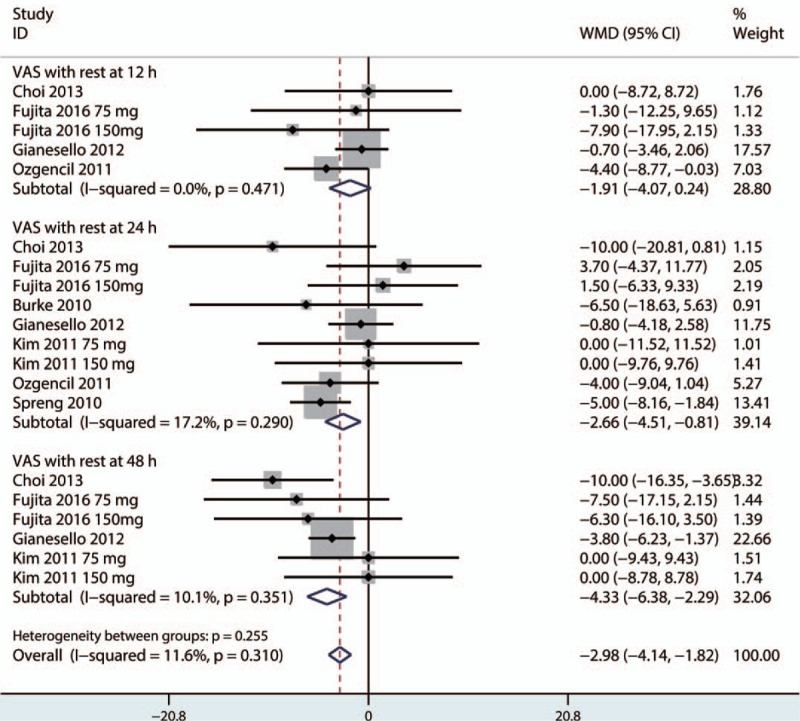
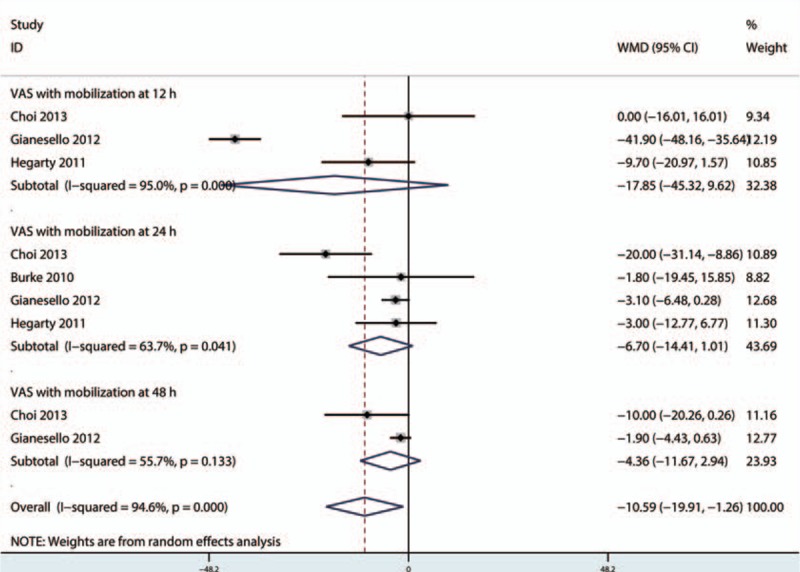
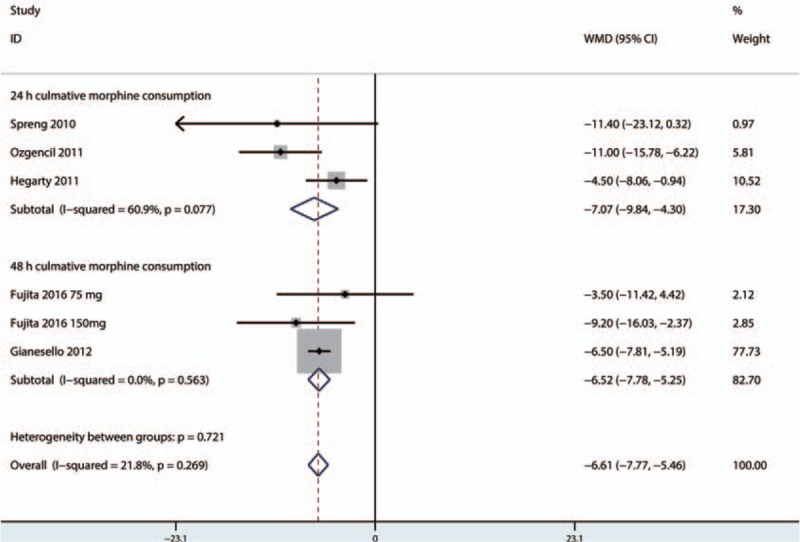
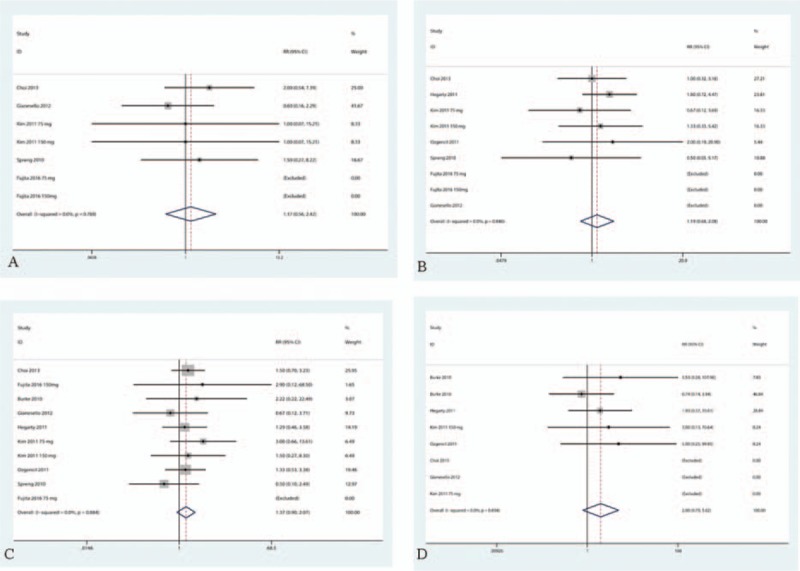
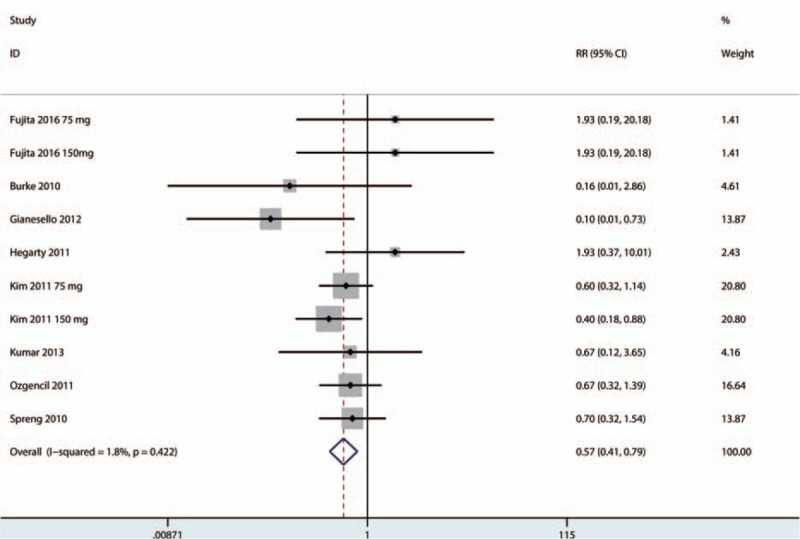
Results: Ten clinical studies with 535 patients (pregabalin group = 294, control group = 241) were included in the meta-analysis. Pregabalin was associated with reduced pain scores at 12 hours, 24 hours, and 48 hours, corresponding to a reduction of 1.91 points (95% CI, -4.07 to 0.24 point) at 12 hours, 2.66 points (95% CI, -4.51 to -0.81 point) at 24 hours, and 4.33 points (95% confidence interval, -6.38 to -2.99 point) at 48 hours on a 100-point numeric rating scale. There was no significant difference between VAS scores with mobilization at 12 hours, 24 hours, or 48 hours. Similarly, pregabalin was associated with a reduction in cumulative morphine consumption at 24 hours (-7.07, 95% CI -9.84, -4.30) and 48 hours (-6.52, 95% CI -7.78, -5.25, P = 0.000). Furthermore, pregabalin can reduce the occurrence of nausea (RR 0.57, 95% CI 0.41, 0.79, P = 0.001, number needed to treat = 8.4). There were no significant differences in the occurrence of sedation, dizziness, headache, or visual disturbances.
Conclusions: Preoperative use of pregabalin was efficacious in reduction of postoperative pain, total morphine consumption, and the occurrence of nausea following spine surgery. Because the sample size and the number of included studies were limited, a multicenter RCT is needed to identify the effects and optimal dose of pregabalin for reducing acute pain after spine surgery.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Pregabalin can decrease acute pain and morphine consumption in laparoscopic cholecystectomy patients: A meta-analysis of randomized controlled trials.Medicine (Baltimore). 2017 May;96(21):e6982. doi: 10.1097/MD.0000000000006982. Medicine (Baltimore). 2017. PMID: 28538404 Free PMC article. Review.
-
A meta-analysis of the preoperative use of gabapentinoids for the treatment of acute postoperative pain following spinal surgery.Medicine (Baltimore). 2017 Sep;96(37):e8031. doi: 10.1097/MD.0000000000008031. Medicine (Baltimore). 2017. PMID: 28906391 Free PMC article.
-
Gabapentin can decrease acute pain and morphine consumption in spinal surgery patients: A meta-analysis of randomized controlled trials.Medicine (Baltimore). 2017 Apr;96(15):e6463. doi: 10.1097/MD.0000000000006463. Medicine (Baltimore). 2017. PMID: 28403075 Free PMC article.
-
The efficacy and safety of ketorolac for postoperative pain management in lumbar spine surgery: a meta-analysis of randomized controlled trials.Syst Rev. 2024 Nov 5;13(1):275. doi: 10.1186/s13643-024-02685-z. Syst Rev. 2024. PMID: 39501393 Free PMC article.
-
Eficacia y seguridad de la analgesia preventiva con gabapentinoides para pacientes sometidos a cirugía artroscópica de hombro: una revisión sistemática y metanálisis.Acta Ortop Mex. 2019 Nov-Dec;33(6):416-423. Acta Ortop Mex. 2019. PMID: 32767888 English.
Cited by
-
Enhanced recovery after elective spinal surgery: an Australian pilot study.J Spine Surg. 2024 Mar 20;10(1):30-39. doi: 10.21037/jss-23-115. Epub 2024 Jan 16. J Spine Surg. 2024. PMID: 38567012 Free PMC article.
-
Pregabalin can decrease acute pain and morphine consumption in laparoscopic cholecystectomy patients: A meta-analysis of randomized controlled trials.Medicine (Baltimore). 2017 May;96(21):e6982. doi: 10.1097/MD.0000000000006982. Medicine (Baltimore). 2017. PMID: 28538404 Free PMC article. Review.
-
Multi-modal pain control regimen for anterior lumbar fusion drastically reduces in-hospital opioid consumption.J Spine Surg. 2020 Dec;6(4):681-687. doi: 10.21037/jss-20-629. J Spine Surg. 2020. PMID: 33447670 Free PMC article.
-
A meta-analysis of the preoperative use of gabapentinoids for the treatment of acute postoperative pain following spinal surgery.Medicine (Baltimore). 2017 Sep;96(37):e8031. doi: 10.1097/MD.0000000000008031. Medicine (Baltimore). 2017. PMID: 28906391 Free PMC article.
-
Preemptive analgesia after lumbar spine surgery by pregabalin and celecoxib: a prospective study.Drug Des Devel Ther. 2019 Jul 3;13:2145-2152. doi: 10.2147/DDDT.S202410. eCollection 2019. Drug Des Devel Ther. 2019. PMID: 31308627 Free PMC article. Clinical Trial.
References
-
- Cohen BE, Hartman MB, Wade JT, et al. Postoperative pain control after lumbar spine fusion. Patient-controlled analgesia versus continuous epidural analgesia. Spine (Phila Pa 1976) 1997;22:1892–6. discussion 1896–1897. - PubMed
-
- Gottschalk A, Freitag M, Tank S, et al. Quality of postoperative pain using an intraoperatively placed epidural catheter after major lumbar spinal surgery. Anesthesiology 2004;101:175–80. - PubMed
-
- Pavlin DJ, Chen C, Penaloza DA, et al. Pain as a factor complicating recovery and discharge after ambulatory surgery. Anesth Analg 2002;95:627–34. table of contents. - PubMed
-
- Yu L, Ran B, Li M, et al. Gabapentin and pregabalin in the management of postoperative pain after lumbar spinal surgery: a systematic review and meta-analysis. Spine (Phila Pa 1976) 2013;38:1947–52. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
