

Radiological prediction of tumor invasiveness of lung adenocarcinoma on thin-section CT
- PMID: 28296757
- PMCID: PMC5369912
- DOI: 10.1097/MD.0000000000006331
Radiological prediction of tumor invasiveness of lung adenocarcinoma on thin-section CT
Abstract
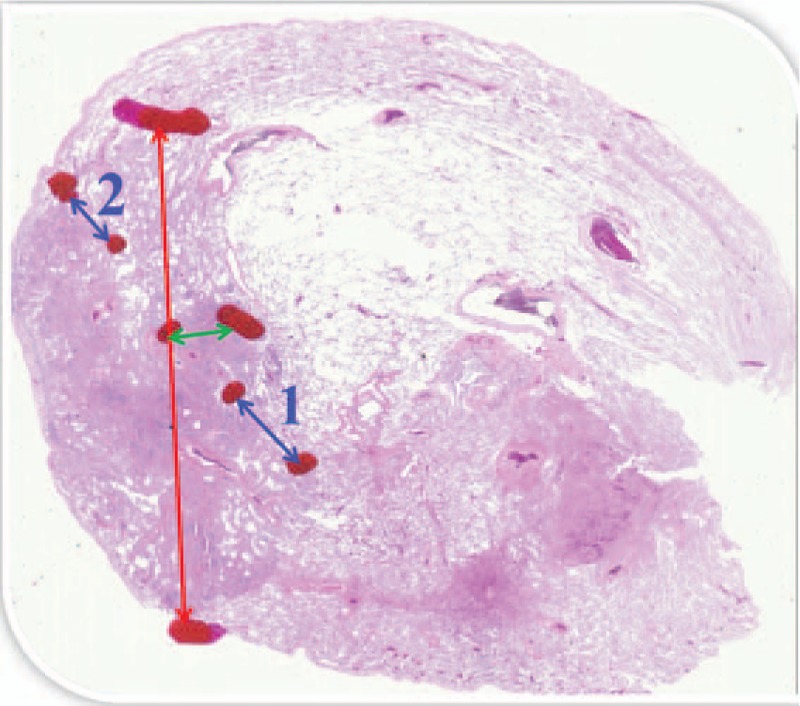
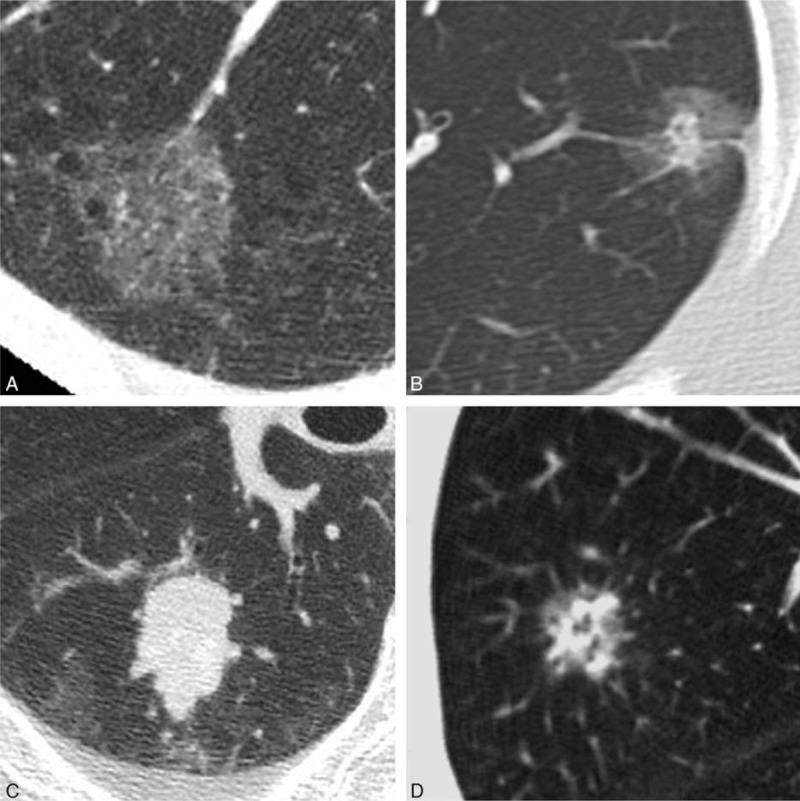
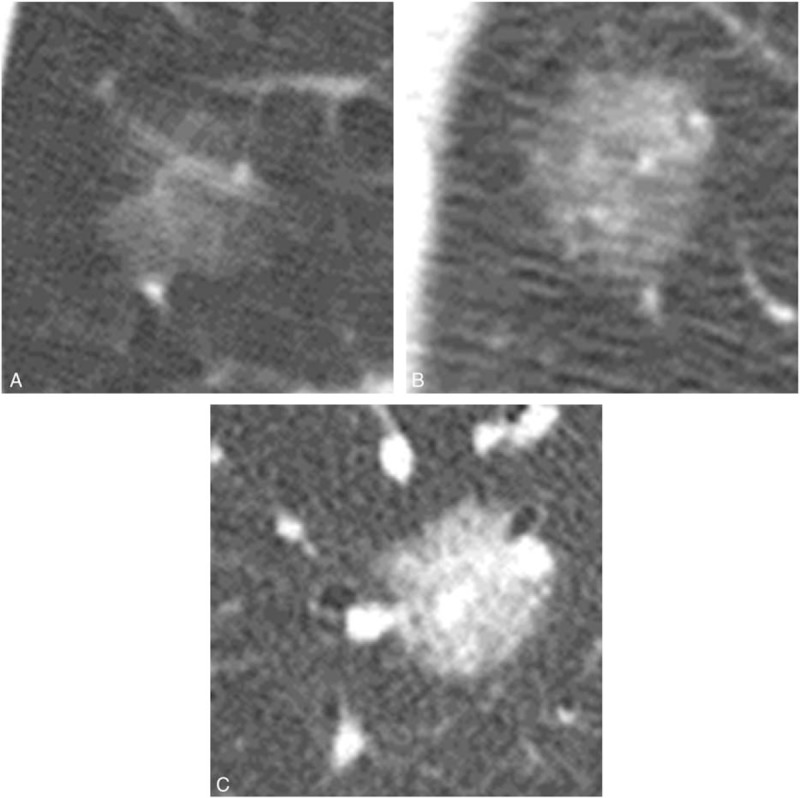
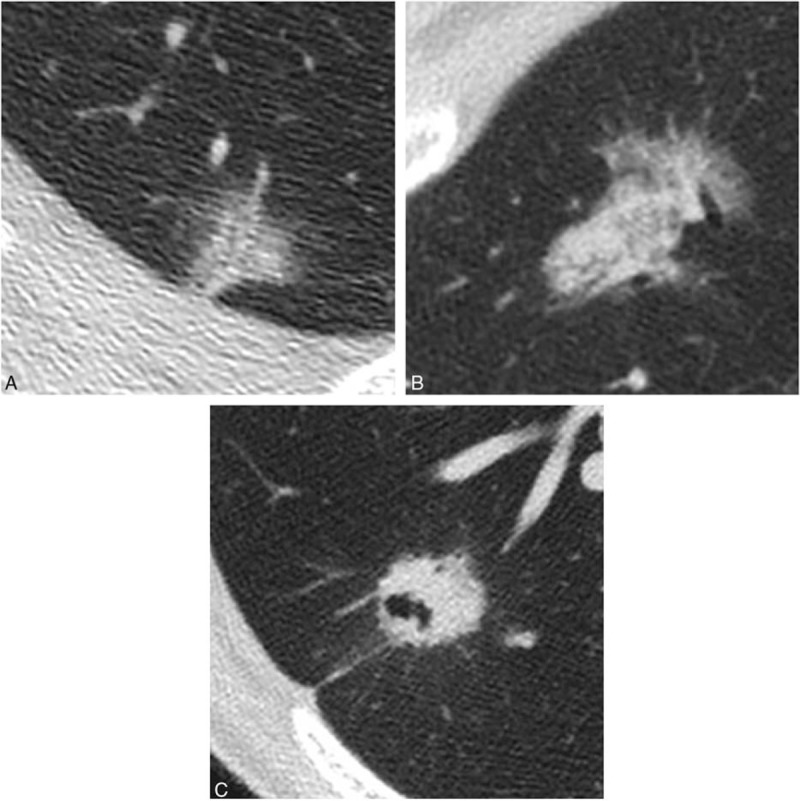
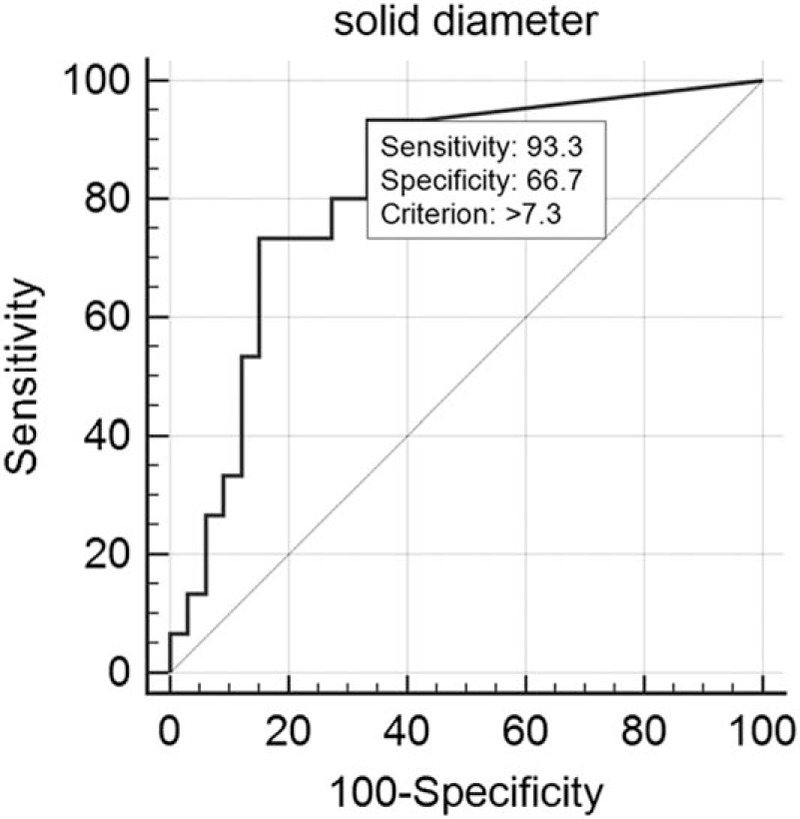
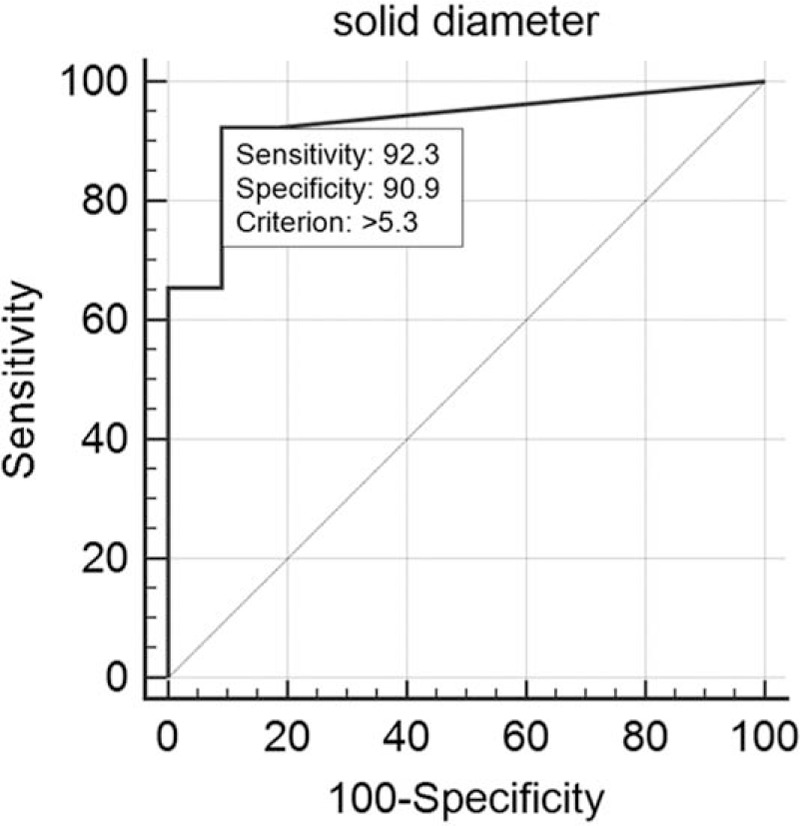
To evaluate thin-section computed tomography (CT) (TSCT) features that differentiate adenocarcinoma in situ (AIS), minimally invasive adenocarcinoma (MIA), and invasive adenocarcinoma (IVA), and to determine the size of solid portion on CT that correlates to pathological invasive components. Forty-eight patients were included. Nodules were classified into ground-glass nodule (GGN), part-solid, solid, and heterogeneous. Visual density of GGNs was subjectively evaluated using reference standard images: faint GGN (Ga), <-700 Hounsfield unit (HU); intermediate GGN (Gb), from -700 to -400 HU; dense GGN (Gc), >-400 HU; and mixed (Ga + Gb, Ga + Gc, and Gb + Gc). The evaluated TSCT findings included margin of nodule, distribution of solid portion, distribution of air bronchiologram, and pleural indentation. The longest diameters of the solid portion and the entire tumor were measured. Invasive diameters were measured in pathological specimens. Twenty-two AISs (16 GGNs [7 Ga, 5 Gb, 2 Gc, 1 Ga + Gc, 1 Gb + Gc], 4 part-solids, and 2 heterogeneous), 6 MIAs (1 GGN [Gb + Gc], 3 part-solids, and 2 solids), and 20 IVAs (1 GGN [Gb], 3 part-solids, and 16 solid) were found. The longest diameter (mean ± standard deviation) of the solid portion and total tumor were 9.7 ± 9.7 and 18.9 ± 5.6 mm, respectively. Significant differences in TSCT findings between AIS and IVA were margin of nodule (Pearson chi-squared test, P = 0.004), distribution of air bronchiologram (P = 0.0148), and pleural indentation (P = 0.0067). A solid portion >5.3 mm on TSCT indicated MIA or IVA, and >7.3 mm indicated IVA (receiver operating characteristic analysis, P < 0.0001). Irregular margin, air bronchiologram with disruption and/or irregular dilatation, and pleural indentation may distinguish IVA from AIS. A 5.3 to 7.3 mm solid portion on TSCT indicates MIA/IVA, and a solid portion >7.3 mm on TSCT indicates IVA.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Lee HJ, Lee CH, Jeong YJ, et al. IASLC/ATS/ERS International Multidisciplinary Classification of Lung Adenocarcinoma: novel concepts and radiologic implications. J Thorac Imaging 2012;27:340–53. - PubMed
-
- Travis WD, Brambilla E, Noguchi M, et al. Diagnosis of lung adenocarcinoma in resected specimens: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification. Arch Pathol Lab Med 2013;137:685–705. - PubMed
-
- Naidich DP, Bankier AA, MacMahon H, et al. Recommendations for the management of subsolid pulmonary nodules detected at CT: a statement from the Fleischner Society. Radiology 2013;266:304–17. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
