

Efficacy and safety of medical therapy for low bone mineral density in patients with Crohn disease: A systematic review with network meta-analysis
- PMID: 28296781
- PMCID: PMC5369936
- DOI: 10.1097/MD.0000000000006378
Efficacy and safety of medical therapy for low bone mineral density in patients with Crohn disease: A systematic review with network meta-analysis
Abstract
Background: Low bone mineral density (BMD) is a frequent complication of inflammatory bowel disease (IBD), particularly in patients with Crohn disease (CD). The aim of our study is to determine the efficacy and safety of different drugs used to treat low BMD in patients with CD.
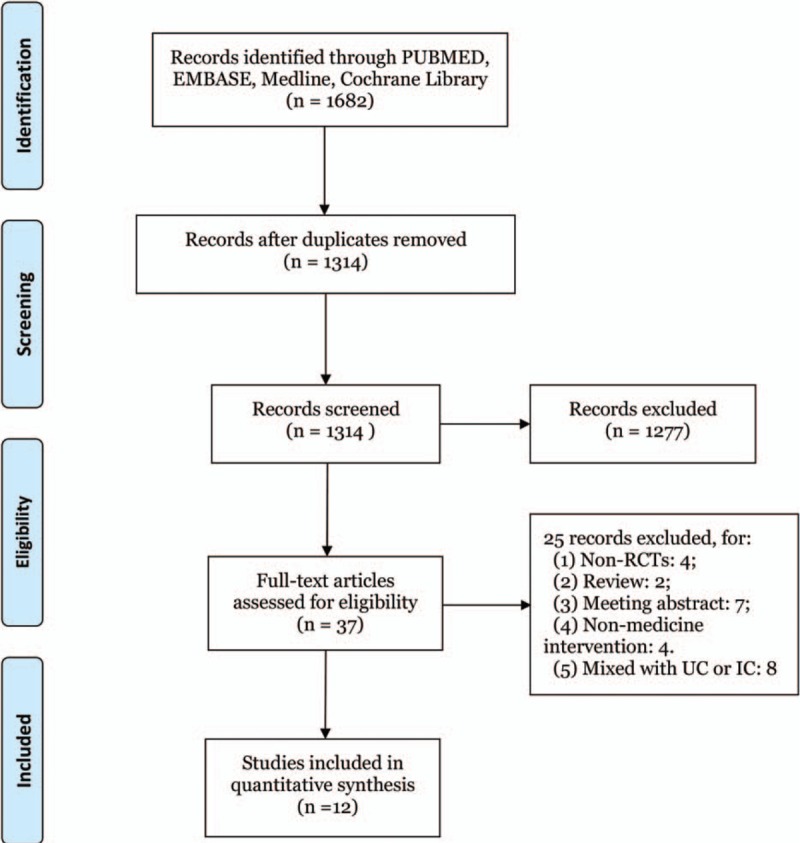
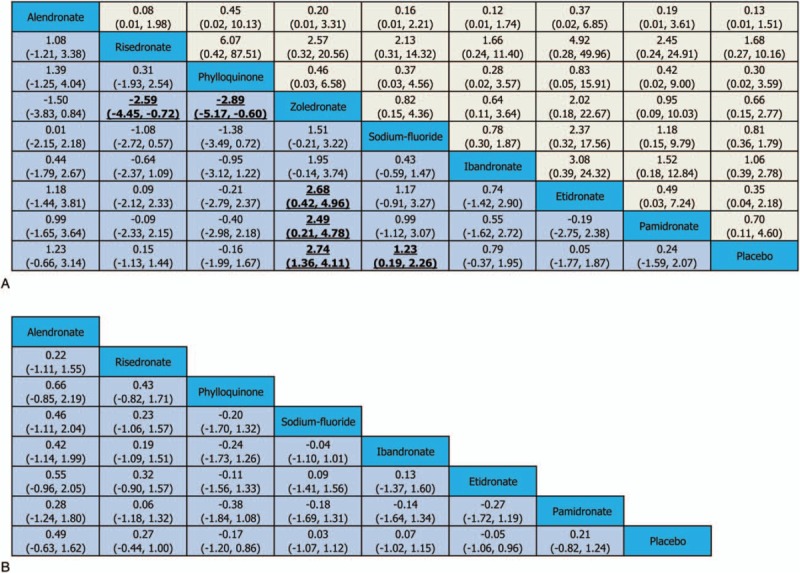
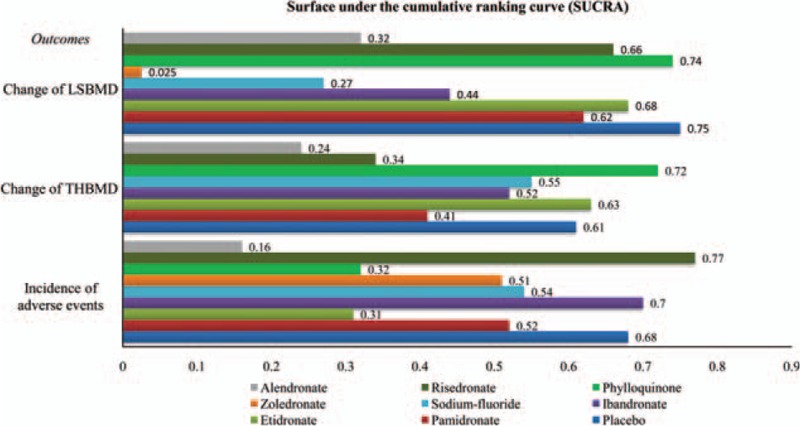
Methods: PUBMED/MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials were searched for eligible studies. A random-effects model within a Bayesian framework was applied to compare treatment effects as standardized mean difference (SMD) with their corresponding 95% credible interval (CrI), while odds ratio (OR) was applied to compare adverse events with 95% CrI. The surface under the cumulative ranking area (SUCRA) was calculated to make the ranking of the treatments for outcomes.
Results: Twelve randomized controlled trials (RCTs) were eligible. Compared with placebo, zoledronate (SMDs 2.74, 95% CrI 1.36-4.11) and sodium-fluoride (SMDs 1.23, 95% CrI 0.19-2.26) revealed statistical significance in increasing lumbar spine BMD (LSBMD). According to SUCRA ranking, zoledronate (SUCRA = 2.5%) might have the highest probability to be the best treatment for increasing LSBMD in CD patients among all agents, followed by sodium-fluoride (27%). For safety assessment, the incidence of adverse events (AEs) demonstrated no statistical difference between agents and placebo. The corresponding SUCRA values indicated that risedronate (SUCRA = 77%) might be the most safe medicine for low BMD in CD patients and alendronate ranked the worst (SUCRA = 16%).
Conclusions: Zoledronate might have the highest probability to be the best therapeutic strategy for increasing LSBMD. For the safety assessment, risedronate showed the greatest trend to decrease the risk of AEs. In the future, more RCTs with higher qualities are needed to make head-to-head comparison between 2 or more treatments.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Bousvaros A, Antonioli DA, Colletti RB, et al. Differentiating ulcerative colitis from Crohn disease in children and young adults: report of a working group of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the Crohn's and Colitis Foundation of America. J Pediatr Gastroenterol Nutr 2007;44:653–74. - PubMed
-
- Cosnes J, Gower-Rousseau C, Seksik P, et al. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology 2011;140:1785–94. - PubMed
-
- Schulte C, Dignass AU, Mann K, et al. Reduced bone mineral density and unbalanced bone metabolism in patients with inflammatory bowel disease. Inflamm Bowel Dis 1998;4:268–75. - PubMed
-
- Von Tirpitz C, Pischulti G, Klaus J, et al. Pathological bone density in chronic inflammatory bowel diseases—prevalence and risk factors. Z Gastroenterol 1999;37:5–12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
