

New-Onset Atrial Fibrillation in the Critically Ill
- PMID: 28296811
- PMCID: PMC5389601
- DOI: 10.1097/CCM.0000000000002325
New-Onset Atrial Fibrillation in the Critically Ill
Abstract
Objective: To determine the association of new-onset atrial fibrillation with outcomes, including ICU length of stay and survival.
Design: Retrospective cohort of ICU admissions. We found atrial fibrillation using automated detection (≥ 90 s in 30 min) and classed as new-onset if there was no prior diagnosis of atrial fibrillation. We identified determinants of new-onset atrial fibrillation and, using propensity matching, characterized its impact on outcomes.
Setting: Tertiary care academic center.
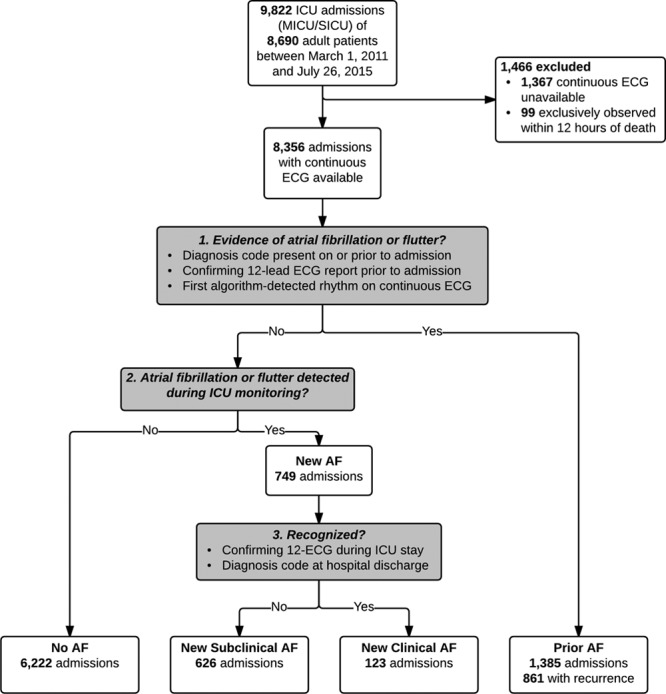
Patients: A total of 8,356 consecutive adult admissions to either the medical or surgical/trauma/burn ICU with available continuous electrocardiogram data.
Interventions: None.
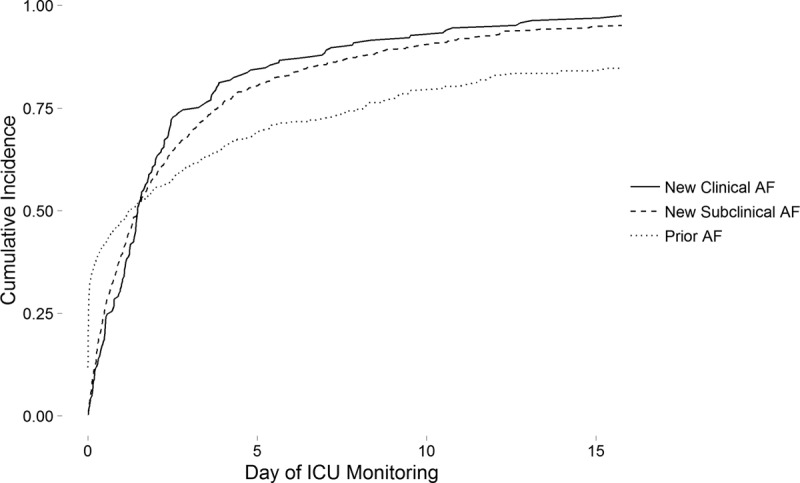
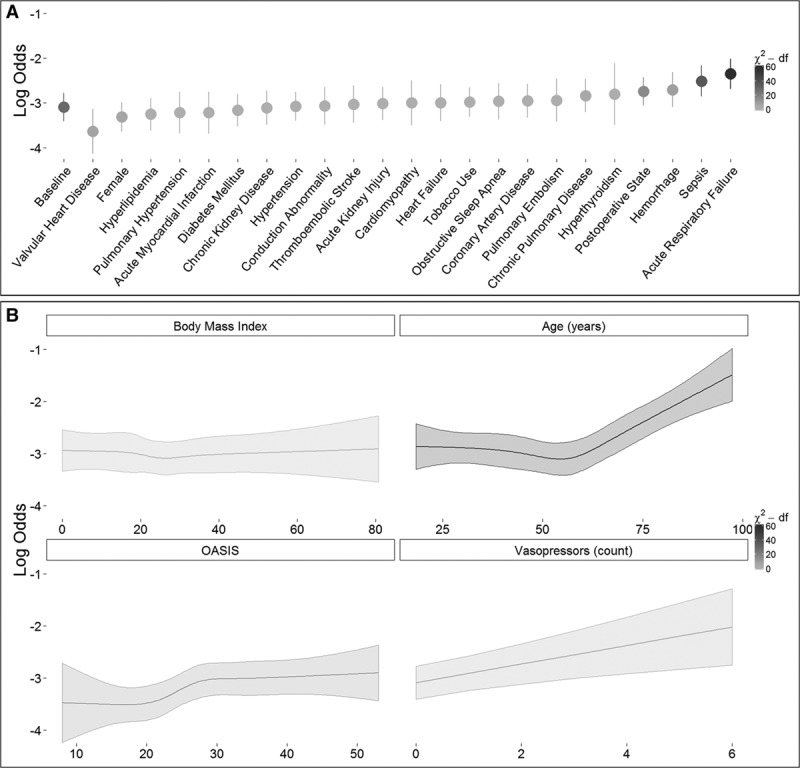
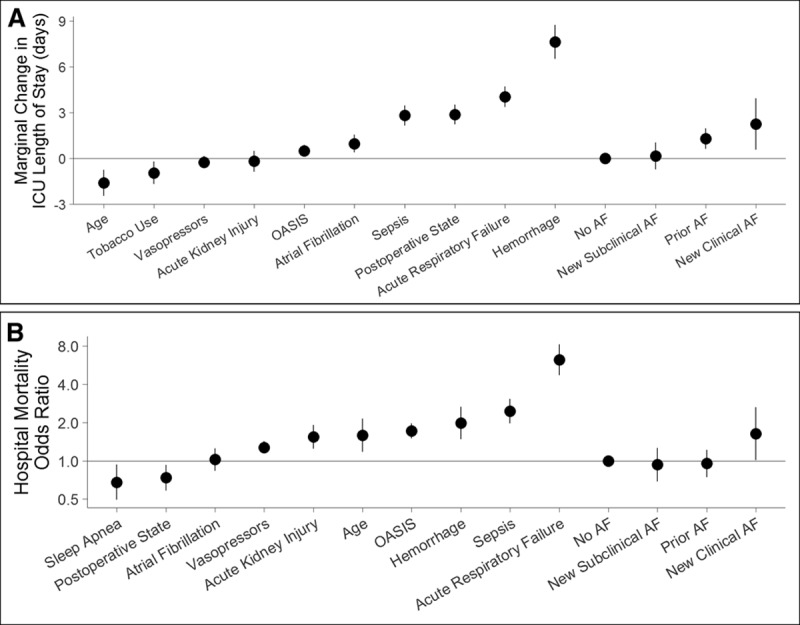
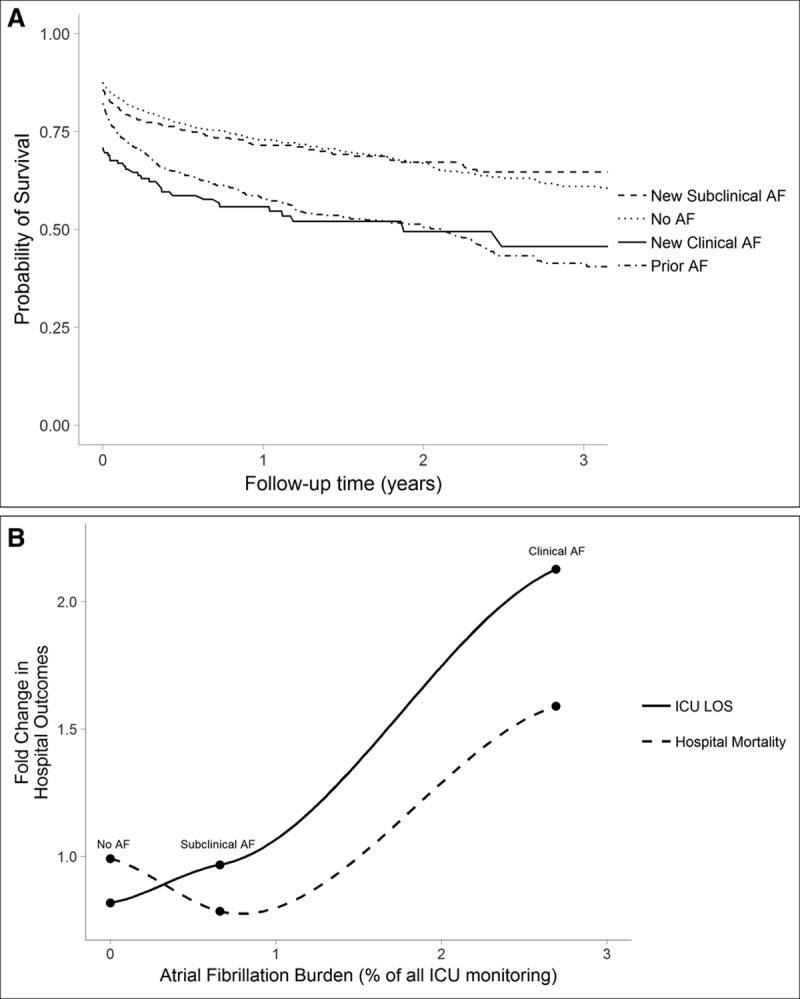
Measurements and main results: From 74 patient-years of every 15-minute observations, we detected atrial fibrillation in 1,610 admissions (19%), with median burden less than 2%. Most atrial fibrillation was paroxysmal; less than 2% of admissions were always in atrial fibrillation. New-onset atrial fibrillation was subclinical or went undocumented in 626, or 8% of all ICU admissions. Advanced age, acute respiratory failure, and sepsis were the strongest predictors of new-onset atrial fibrillation. In propensity-adjusted regression analyses, clinical new-onset atrial fibrillation was associated with increased hospital mortality (odds ratio, 1.63; 95% CI, 1.01-2.63) and longer length of stay (2.25 d; CI, 0.58-3.92). New-onset atrial fibrillation was not associated with survival after hospital discharge (hazard ratio, 0.99; 95% CI, 0.76-1.28 and hazard ratio, 1.11; 95% CI, 0.67-1.83, respectively, for subclinical and clinical new-onset atrial fibrillation).
Conclusions: Automated analysis of continuous electrocardiogram heart rate dynamics detects new-onset atrial fibrillation in many ICU patients. Though often transient and frequently unrecognized, new-onset atrial fibrillation is associated with poor hospital outcomes.
Conflict of interest statement
Dr. Moorman received funding from Advanced Medical Predictive Devices, Diagnostics, and Displays. He owns equity and is Chief Medical Officer of Advanced Medical Predictive Devices, Diagnostics, and Displays in Charlottesville, VA, which has licensed related technologies from the University of Virginia Licensing and Ventures Group. For several months in 2015, he received consulting fees. His wife Liza is Clinical Implementation Officer of Advanced Medical Predictive Devices, Diagnostics, and Displays. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Will Artificial Intelligence Contribute to Overuse in Healthcare?Crit Care Med. 2017 May;45(5):912-913. doi: 10.1097/CCM.0000000000002351. Crit Care Med. 2017. PMID: 28410309 Free PMC article. No abstract available.
-
An Overlook of New-Onset Atrial Fibrillation in the Critically Ill Using Automated Detection: Have We Over Looked at It?Crit Care Med. 2017 Nov;45(11):e1195. doi: 10.1097/CCM.0000000000002617. Crit Care Med. 2017. PMID: 29028721 No abstract available.
-
The authors reply.Crit Care Med. 2017 Nov;45(11):e1195-e1196. doi: 10.1097/CCM.0000000000002664. Crit Care Med. 2017. PMID: 29028722 Free PMC article. No abstract available.
References
-
- Kanji S, Williamson DR, Yaghchi BM, et al. Canadian Critical Care Trials Group: Epidemiology and management of atrial fibrillation in medical and noncardiac surgical adult intensive care unit patients. J Crit Care 2012; 27:326.e1–326.e8 - PubMed
-
- LaPar DJ, Speir AM, Crosby IK, et al. Postoperative atrial fibrillation significantly increases mortality, hospital readmission, and hospital costs. Ann Thorac Surg 2014; 98:527–533 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
