

Prevalence of chronic kidney disease and risk factors for its progression: A cross-sectional comparison of Indians living in Indian versus U.S. cities
- PMID: 28296920
- PMCID: PMC5351850
- DOI: 10.1371/journal.pone.0173554
Prevalence of chronic kidney disease and risk factors for its progression: A cross-sectional comparison of Indians living in Indian versus U.S. cities
Abstract
Background: While data from the latter part of the twentieth century consistently showed that immigrants to high-income countries faced higher cardio-metabolic risk than their counterparts in low- and middle-income countries, urbanization and associated lifestyle changes may be changing these patterns, even for conditions considered to be advanced manifestations of cardio-metabolic disease (e.g., chronic kidney disease [CKD]).
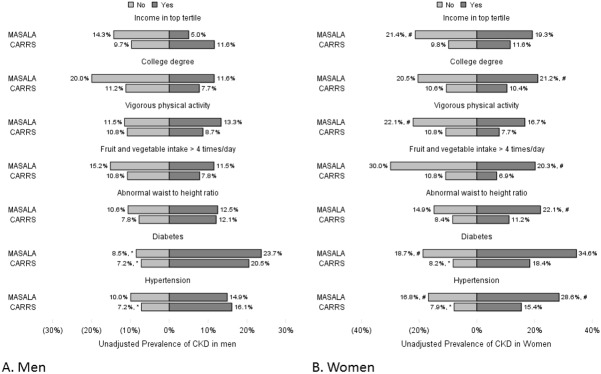
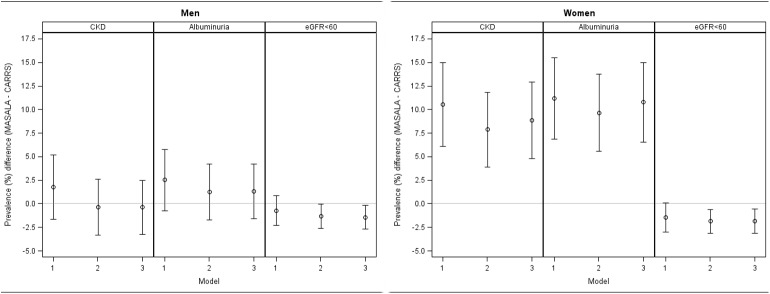
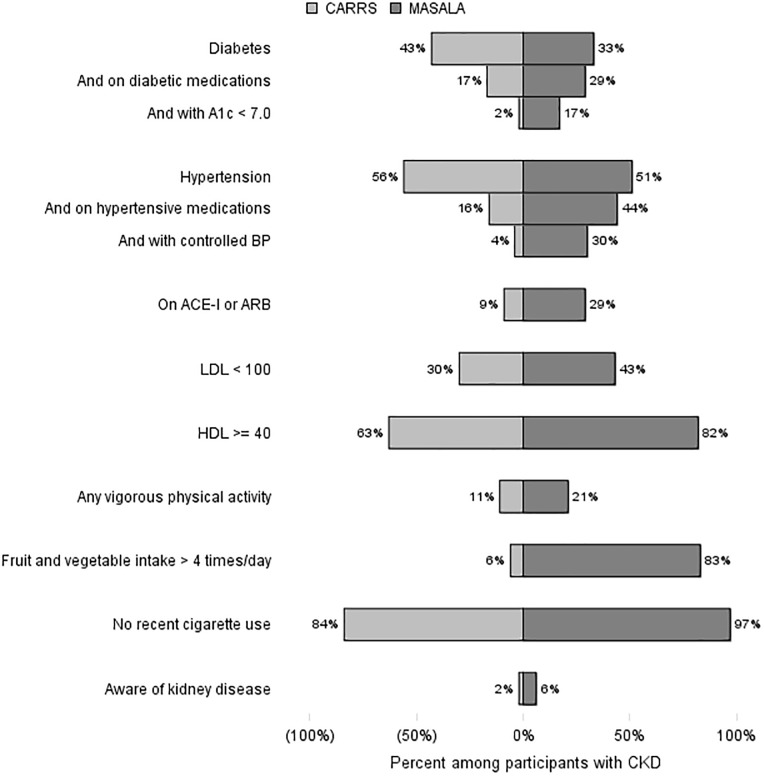
Methods and findings: Using cross-sectional data from the Center for cArdiometabolic Risk Reduction in South Asia (CARRS, n = 5294) and Mediators of Atherosclerosis in South Asians Living in America (MASALA, n = 748) studies, we investigated whether prevalence of CKD is similar among Indians living in Indian and U.S. cities. We compared crude, age-, waist-to-height ratio-, and diabetes- adjusted CKD prevalence difference. Among participants identified to have CKD, we compared management of risk factors for its progression. Overall age-adjusted prevalence of CKD was similar in MASALA (14.0% [95% CI 11.8-16.3]) compared with CARRS (10.8% [95% CI 10.0-11.6]). Among men the prevalence difference was low (prevalence difference 1.8 [95% CI -1.6,5.3]) and remained low after adjustment for age, waist-to-height ratio, and diabetes status (-0.4 [-3.2,2.5]). Adjusted prevalence difference was higher among women (prevalence difference 8.9 [4.8,12.9]), but driven entirely by a higher prevalence of albuminuria among women in MASALA. Severity of CKD--i.e., degree of albuminuria and proportion of participants with reduced glomerular filtration fraction--was higher in CARRS for both men and women. Fewer participants with CKD in CARRS were effectively treated. 4% of CARRS versus 51% of MASALA participants with CKD had A1c < 7%; and 7% of CARRS versus 59% of MASALA participants blood pressure < 140/90 mmHg. Our analysis applies only to urban populations. Demographic--particularly educational attainment--differences among participants in the two studies are a potential source of bias.
Conclusions: Prevalence of CKD among Indians living in Indian and U.S. cities is similar. Persons with CKD living in Indian cities face higher likelihood of experiencing end-stage renal disease since they have more severe kidney disease and little evidence of risk factor management.
Conflict of interest statement
Figures
References
-
- Luke A, Durazo-Arvizu R, Rotimi C, Prewitt TE, Forrester T, Wilks R, et al. Relation between body mass index and body fat in black population samples from Nigeria, Jamaica, and the United States. American journal of epidemiology. 1997;145(7):620–8. - PubMed
-
- Bhatnagar D, Anand IS, Durrington PN, Patel DJ, Wander GS, Mackness MI, et al. Coronary risk factors in people from the Indian subcontinent living in west London and their siblings in India. Lancet. 1995;345(8947):405–9. - PubMed
-
- Robertson TL, Kato H, Rhoads GG, Kagan A, Marmot M, Syme SL, et al. Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California. Incidence of myocardial infarction and death from coronary heart disease. The American journal of cardiology. 1977;39(2):239–43. - PubMed
-
- Gujral UP, Narayan KM, Pradeepa RG, Deepa M, Ali MK, Anjana RM, et al. Comparing Type 2 Diabetes, Prediabetes, and Their Associated Risk Factors in Asian Indians in India and in the U.S.: The CARRS and MASALA Studies. Diabetes care. 2015;38(7):1312–8. PubMed Central PMCID: PMC4477335. 10.2337/dc15-0032 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
