

Computer assisted electromagnetic navigation improves accuracy in computed tomography guided interventions: A prospective randomized clinical trial
- PMID: 28296957
- PMCID: PMC5351986
- DOI: 10.1371/journal.pone.0173751
Computer assisted electromagnetic navigation improves accuracy in computed tomography guided interventions: A prospective randomized clinical trial
Abstract
Purpose: To assess the accuracy and usability of an electromagnetic navigation system designed to assist Computed Tomography (CT) guided interventions.
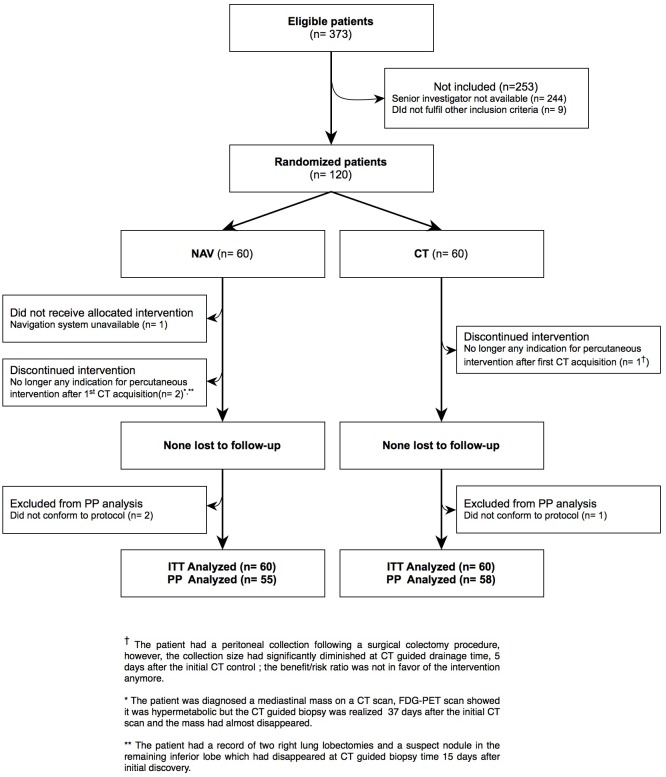
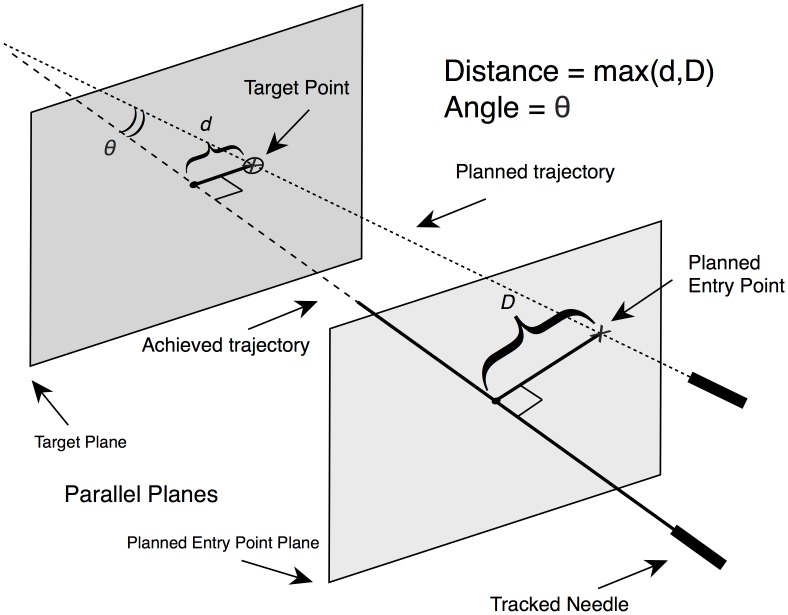
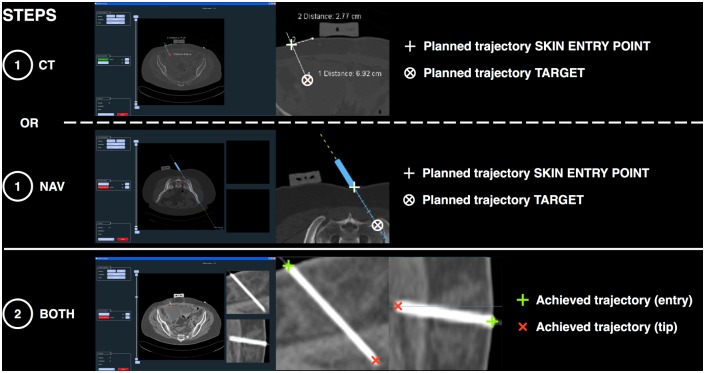
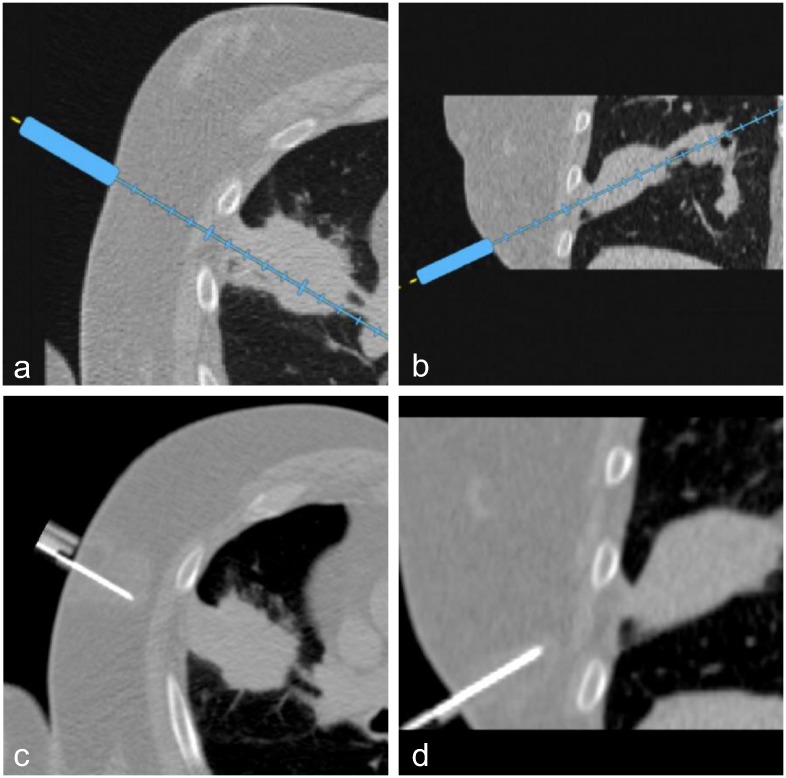
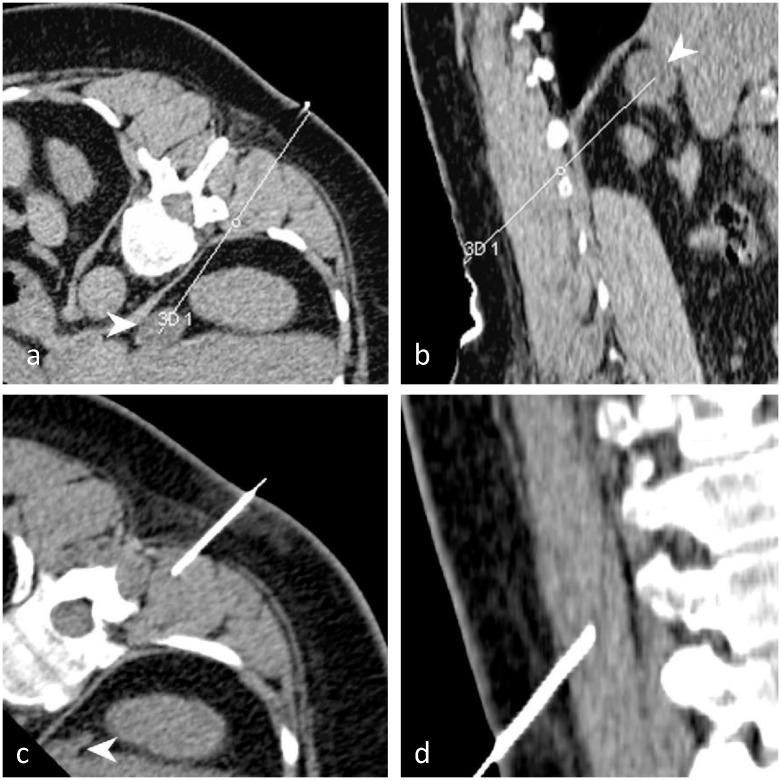
Materials and methods: 120 patients requiring a percutaneous CT intervention (drainage, biopsy, tumor ablation, infiltration, sympathicolysis) were included in this prospective randomized trial. Nineteen radiologists participated. Conventional procedures (CT group) were compared with procedures assisted by a navigation system prototype using an electromagnetic localizer to track the position and orientation of a needle holder (NAV group). The navigation system displays the needle path in real-time on 2D reconstructed CT images extracted from the 3D CT volume. The regional ethics committee approved this study and all patients gave written informed consent. The main outcome was the distance between the planned trajectory and the achieved needle trajectory calculated from the initial needle placement.
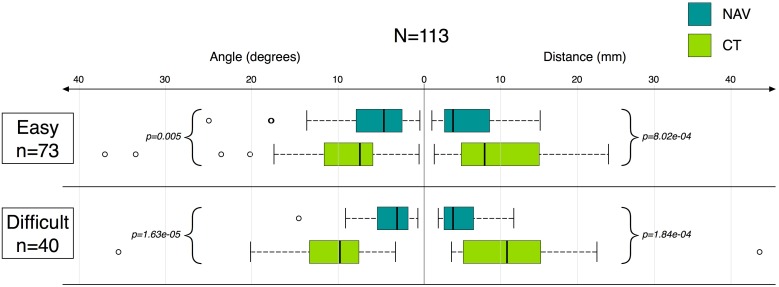
Results: 120 patients were analyzable in intention-to-treat (NAV: 60; CT: 60). Accuracy improved when the navigation system was used: distance error (in millimeters: median[P25%; P75%]) with NAV = 4.1[2.7; 9.1], vs. with CT = 8.9[4.9; 15.1] (p<0.001). After the initial needle placement and first control CT, fewer subsequent CT acquisitions were necessary to reach the target using the navigation system: NAV = 2[2; 3]; CT = 3[2; 4] (p = 0.01).
Conclusion: The tested system was usable in a standard clinical setting and provided significant improvement in accuracy; furthermore, with the help of navigation, targets could be reached with fewer CT control acquisitions.
Conflict of interest statement
Figures

References
-
- Arnolli MM, Hanumara NC, Franken M, Broeders IAMJ. An overview of systems for CT- and MRI-guided percutaneous needle placement in the thorax and abdomen. Int J Med Robotics Comput Assist Surg. 2015. December; 11(4): 458–75. - PubMed
-
- Grasso R, Faiella E, Luppi G, Schena E, Giurazza F, Del Vescovo R, et al. Percutaneous lung biopsy: comparaison between an augmented reality CT navigation system and standard Ct-guided technique. Int. J. Comput. Assist. Radiol. Surg. 2013. September 5; 8:837–848. 10.1007/s11548-013-0816-8 - DOI - PubMed
-
- Grand D, Atalay M, Cronan J, Mayo-Smith W, Dupuy D. CT-guided percuntaneous lung biopsy: comparison of conventional CT fluoroscopy to CT fluoroscopy with electromagnetic navigation system in 60 consecutive patients. European journal of radiology. 2011. August 2;79:133–136. - PubMed
-
- Imactis CT-Navigation. [Online] [Cited: June30, 2015.]. http://www.imactis.com/index.php?module=produit&language=en_EN&PHPSESSID...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
