

Clinicopathologic, Immunohistochemical, and Molecular Features of Histiocytoid Sweet Syndrome
- PMID: 28296991
- PMCID: PMC5543327
- DOI: 10.1001/jamadermatol.2016.6092
Clinicopathologic, Immunohistochemical, and Molecular Features of Histiocytoid Sweet Syndrome
Abstract
Importance: Histiocytoid Sweet syndrome is a rare histopathologic variant of Sweet syndrome. The nature of the histiocytoid infiltrate has generated considerable controversy in the literature.
Objective: The main goal of this study was to conduct a comprehensive overview of the immunohistochemical phenotype of the infiltrate in histiocytoid Sweet syndrome. We also analyze whether this variant of Sweet syndrome is more frequently associated with hematologic malignancies than classic Sweet syndrome.
Design: This is a retrospective case series study of the clinicopathologic, immunohistochemical, and molecular features of 33 patients with a clinicopathologic diagnosis of histiocytoid Sweet syndrome was conducted in the dermatology departments of 5 university hospitals and a private laboratory of dermatopathology.
Main outcome and measures: The clinical, histopathological, immunohistochemical, and follow-up features of 33 patients with histiocytoid Sweet syndrome were analyzed. In some cases, cytogenetic studies of the dermal infiltrate were also performed. We compare our findings with those of the literature.
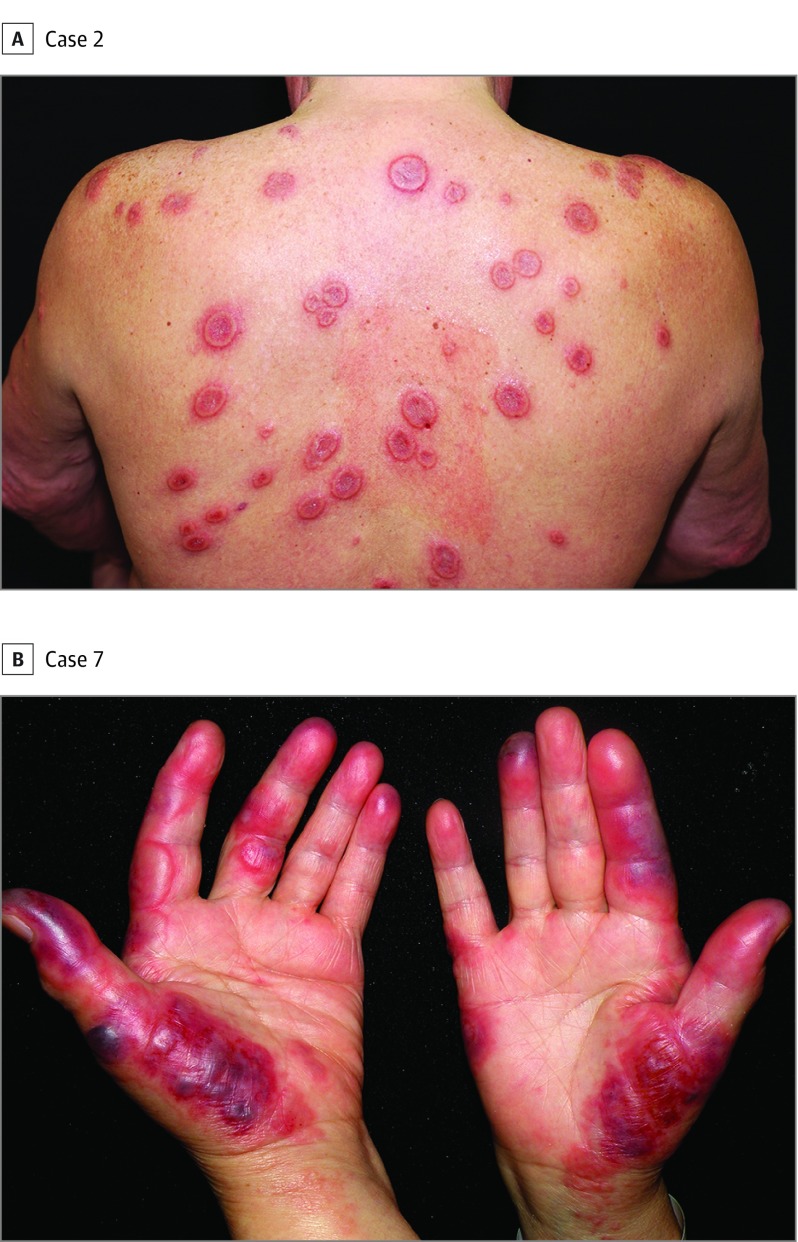
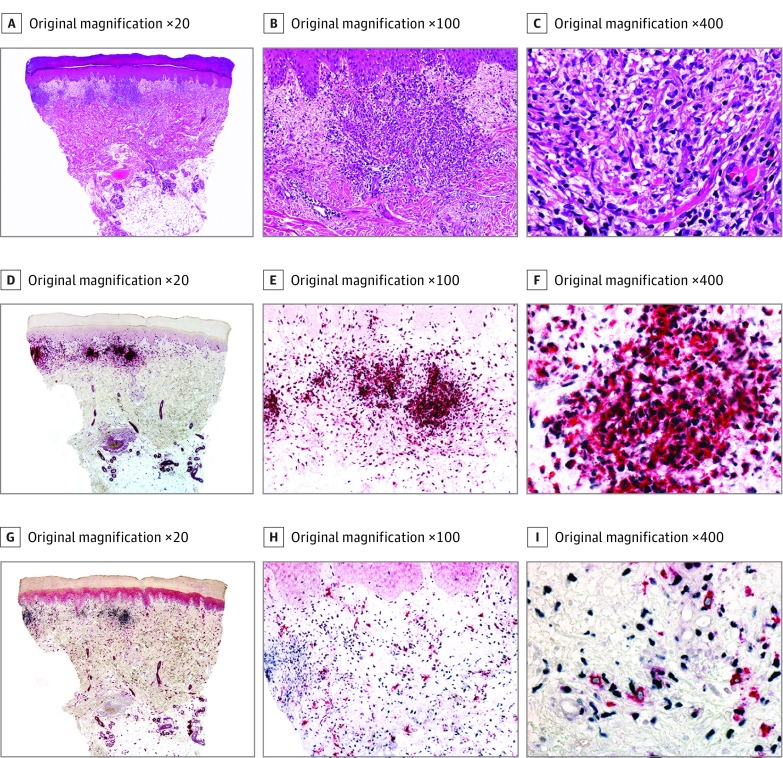
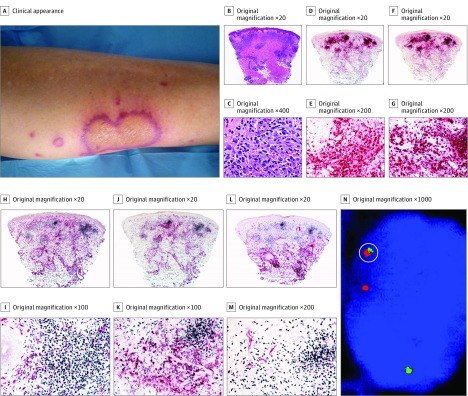
Results: The dermal infiltrate from the 33 study patients (20 female; median age, 49 years; age range, 5-93 years; and 13 male; median age, 42 years; age range, 4-76 years) was mainly composed of myeloperoxidase-positive immature myelomonocytic cells with histiocytoid morphology. No cytogenetic anomalies were found in the infiltrate except in 1 case in which neoplastic cells of chronic myelogenous leukemia were intermingled with the cells of histiocytoid Sweet syndrome. Authentic histiocytes were also found in most cases, with a mature immunoprofile, but they appeared to be a minor component of the infiltrate. Histiocytoid Sweet syndrome was not more frequently related with hematologic malignancies than classic neutrophilic Sweet syndrome.
Conclusions and relevance: The dermal infiltrate of cutaneous lesions of histiocytoid Sweet syndrome is composed mostly of immature cells of myeloid lineage. This infiltrate should not be interpreted as leukemia cutis.
Conflict of interest statement
Figures
Comment in
-
Histiocytoid Sweet Syndrome and Myelodysplastic Syndrome.JAMA Dermatol. 2017 Aug 1;153(8):835-836. doi: 10.1001/jamadermatol.2017.1669. JAMA Dermatol. 2017. PMID: 28614548 No abstract available.
-
Histiocytoid Sweet Syndrome and Myelodysplastic Syndrome-Reply.JAMA Dermatol. 2017 Aug 1;153(8):836-837. doi: 10.1001/jamadermatol.2017.1670. JAMA Dermatol. 2017. PMID: 28614552 No abstract available.
References
-
- Requena L, Kutzner H, Palmedo G, et al. Histiocytoid Sweet syndrome: a dermal infiltration of immature neutrophilic granulocytes. Arch Dermatol. 2005;141(7):834-842. - PubMed
-
- Kim JS, Roh HS, Lee JW, Lee MW, Yu HJ. Distinct variant of Sweet’s syndrome: bortezomib-induced histiocytoid Sweet’s syndrome in a patient with multiple myeloma. Int J Dermatol. 2012;51(12):1491-1493. - PubMed
-
- Wu AJ, Rodgers T, Fullen DR. Drug-associated histiocytoid Sweet’s syndrome: a true neutrophilic maturation arrest variant. J Cutan Pathol. 2008;35(2):220-224. - PubMed
-
- Murase JE, Wu JJ, Theate I, Cole GW, Barr RJ, Dyson SW. Bortezomib-induced histiocytoid Sweet syndrome. J Am Acad Dermatol. 2009;60(3):496-497. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
