

Use of Computerized Clinical Decision Support Systems to Prevent Venous Thromboembolism in Surgical Patients: A Systematic Review and Meta-analysis
- PMID: 28297002
- PMCID: PMC5831455
- DOI: 10.1001/jamasurg.2017.0131
Use of Computerized Clinical Decision Support Systems to Prevent Venous Thromboembolism in Surgical Patients: A Systematic Review and Meta-analysis
Abstract
Importance: Health care professionals do not adequately stratify risk or provide prophylaxis for venous thromboembolism (VTE) among surgical patients. Computerized clinical decision support systems (CCDSSs) have been implemented to assist clinicians and improve prophylaxis for VTE.
Objective: To evaluate the effect of implementing CCDSSs on the ordering of VTE prophylaxis and the rates of VTE.
Data sources: PubMed, MEDLINE via OVID, EMBASE via OVID, Scopus, Cochrane CENTRAL Register of Controlled Trials, and clinicaltrials.gov were searched in June 2016 for articles published in English from October 15, 1991, to February 16, 2016. A manual search of references from relevant articles was also performed.
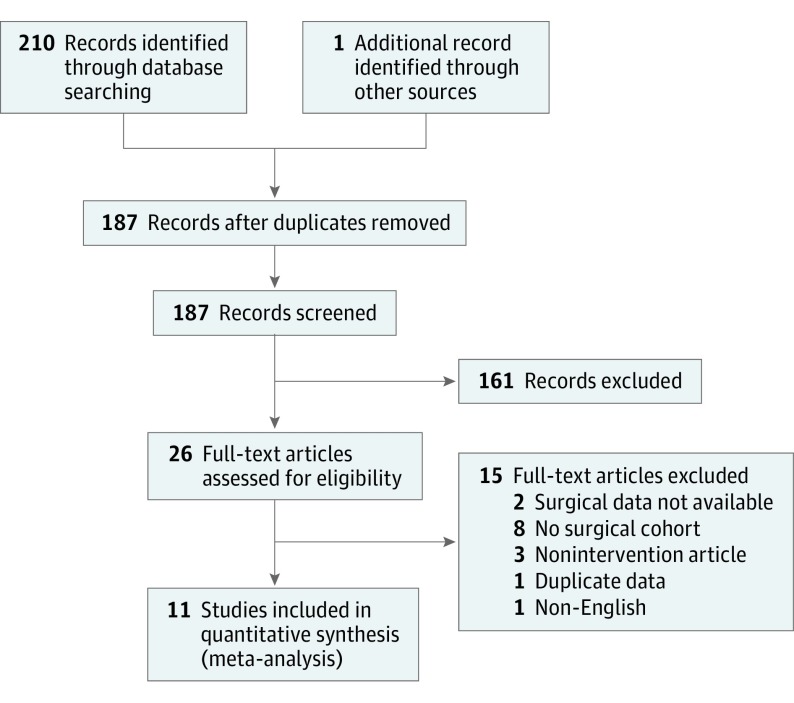
Study selection: Clinical trials and observational studies among surgical patients comparing CCDSSs with VTE risk stratification and assistance in ordering prophylaxis vs routine care without decision support were included. Of the 188 articles screened, 11 (5.9%) were eligible for meta-analysis.
Data extraction and synthesis: Meta-analysis of Observational Studies in Epidemiology guidelines were followed. Two reviewers extracted data and assessed quality independently.
Main outcomes and measures: Rates of prophylaxis for VTE and VTE events. Random- and fixed-effects models were used to summarize odds ratios and risk ratios.
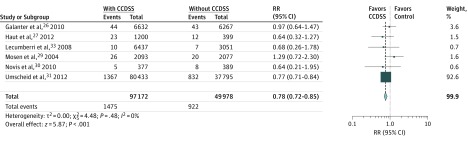
Results: Eleven articles (9 prospective cohort trials and 2 retrospective cohort trials) comprising 156 366 individuals (104 241 in the intervention group and 52 125 in the control group) were included. The use of CCDSSs was associated with a significant increase in the rate of appropriate ordering of prophylaxis for VTE (odds ratio, 2.35; 95% CI, 1.78-3.10; P < .001) and a significant decrease in the risk of VTE events (risk ratio, 0.78; 95% CI, 0.72-0.85; P < .001).
Conclusions and relevance: Use of CCDSSs increases the proportion of surgical patients who were prescribed adequate prophylaxis for VTE and correlates with a reduction in VTE events.
Conflict of interest statement
Figures
Comment in
-
Computerized Clinical Decision Support Systems for Prevention of Venous Thromboembolism: Why Can't My Electronic Health Record Be More Like Netflix, Amazon, Google, and Apple?JAMA Surg. 2017 Jul 1;152(7):646-647. doi: 10.1001/jamasurg.2017.0107. JAMA Surg. 2017. PMID: 28297010 No abstract available.
References
-
- Geerts WH, Bergqvist D, Pineo GF, et al. ; American College of Chest Physicians . Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6)(suppl):381S-453S. - PubMed
-
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3)(suppl):338S-400S. - PubMed
-
- Bahl V, Shuman AG, Hu HM, et al. Chemoprophylaxis for venous thromboembolism in otolaryngology. JAMA Otolaryngol Head Neck Surg. 2014;140(11):999-1005. - PubMed
-
- Bergqvist D, Agnelli G, Cohen AT, et al. ; ENOXACAN II Investigators . Duration of prophylaxis against venous thromboembolism with enoxaparin after surgery for cancer. N Engl J Med. 2002;346(13):975-980. - PubMed
-
- Kukreja JE, Levey HR, Scosyrev E, et al. Effectiveness and safety of extended-duration prophylaxis for venous thromboembolism in major urologic oncology surgery. Urol Oncol. 2015;33(9):387.e7-387.e16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
