

Bystander Defibrillation for Out-of-Hospital Cardiac Arrest in Public vs Residential Locations
- PMID: 28297003
- PMCID: PMC5814985
- DOI: 10.1001/jamacardio.2017.0008
Bystander Defibrillation for Out-of-Hospital Cardiac Arrest in Public vs Residential Locations
Abstract
Importance: Bystander-delivered defibrillation (hereinafter referred to as bystander defibrillation) of patients with out-of-hospital cardiac arrests (OHCAs) remains limited despite the widespread dissemination of automated external defibrillators (AEDs).
Objective: To examine calendar changes in bystander defibrillation and subsequent survival according to a public or a residential location of the cardiac arrest after nationwide initiatives in Denmark to facilitate bystander-mediated resuscitative efforts, including bystander defibrillation.
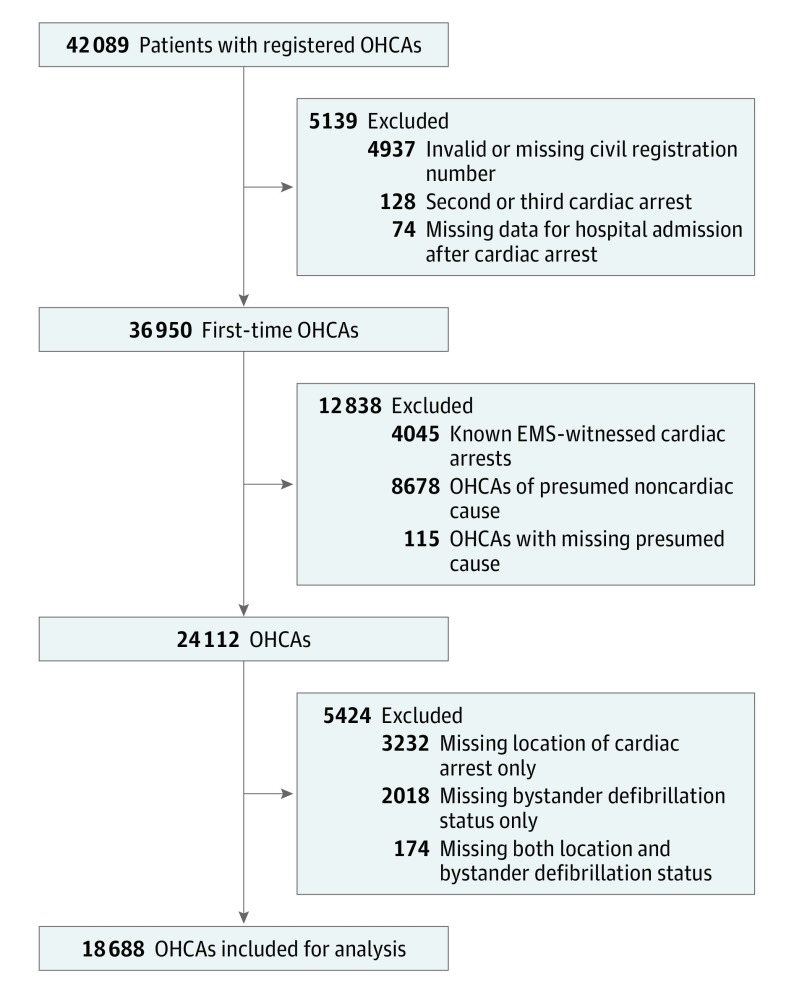
Design, setting, and participants: This nationwide study identified 18 688 patients in Denmark with first-time OHCA from June 1, 2001, to December 31, 2012, using the Danish Cardiac Arrest Registry. Patients had a presumed cardiac cause of arrest that was not witnessed by emergency medical services personnel. Data were analyzed from April 1, 2015, to December 10, 2016.
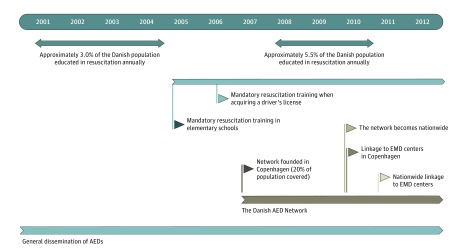
Exposures: Nationwide initiatives to facilitate bystander resuscitative efforts, including bystander defibrillation, consisted of resuscitation training of Danish citizens, dissemination of on-site AEDs, foundation of an AED registry linked to emergency medical dispatch centers, and dispatcher-assisted guidance of bystander resuscitation efforts.
Main outcomes and measures: The proportion of patients who received bystander defibrillation according to the location of the cardiac arrest and their subsequent 30-day survival.
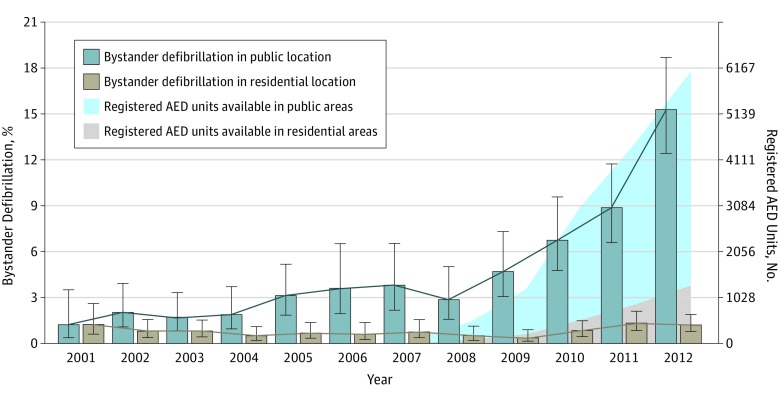
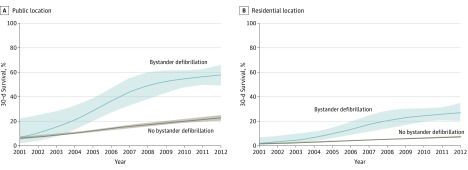
Results: Of the 18 688 patients with OHCAs (67.8% men and 32.2% women; median [interquartile range] age, 72 [62-80] years), 4783 (25.6%) had a cardiac arrest in a public location and 13 905 (74.4%) in a residential location. The number of registered AEDs increased from 141 in 2007 to 7800 in 2012. The distribution of AED location was consistently skewed in favor of public locations. Bystander defibrillation increased in public locations from 3 of 245 (1.2%; 95% CI, 0.4%-3.5%) in 2001 to 78 of 510 (15.3%; 95% CI, 12.4%-18.7%) in 2012 (P < .001) but remained unchanged in residential locations from 7 of 542 (1.3%; 95% CI, 0.6%-2.6%) in 2001 to 21 of 1669 (1.3%; 95% CI, 0.8%-1.9%) in 2012 (P = .17). Thirty-day survival after bystander defibrillation increased in public locations from 8.3% (95% CI, 1.5%-35.4%) in 2001/2002 to 57.5% (95% CI, 48.6%-66.0%) in 2011/2012 (P < .001) in residential locations, from 0.0% (95% CI, 0.0%-19.4%) in 2001/2002 to 25.6% (95% CI, 14.6%-41.1%) in 2011/2012 (P < .001).
Conclusions and relevance: Initiatives to facilitate bystander defibrillation were associated with a marked increase in bystander defibrillation in public locations, whereas bystander defibrillation remained limited in residential locations. Concomitantly, survival increased after bystander defibrillation in residential and public locations.
Conflict of interest statement
Figures
Comment in
-
Cardiac Arrest in Any Location: The Need for Fewer Bystanders and More Layperson Rescuers.JAMA Cardiol. 2017 May 1;2(5):514-515. doi: 10.1001/jamacardio.2017.0040. JAMA Cardiol. 2017. PMID: 28297005 No abstract available.
References
-
- Caffrey SL, Willoughby PJ, Pepe PE, Becker LB. Public use of automated external defibrillators. N Engl J Med. 2002;347(16):1242-1247. - PubMed
-
- Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomes of rapid defibrillation by security officers after cardiac arrest in casinos. N Engl J Med. 2000;343(17):1206-1209. - PubMed
-
- Page RL, Joglar JA, Kowal RC, et al. Use of automated external defibrillators by a US airline. N Engl J Med. 2000;343(17):1210-1216. - PubMed
-
- Kitamura T, Kiyohara K, Sakai T, et al. Public-access defibrillation and out-of-hospital cardiac arrest in Japan. N Engl J Med. 2016;375(17):1649-1659. - PubMed
-
- Link MS, Atkins DL, Passman RS, et al. 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care: part 6: electrical therapies: automated external defibrillators, defibrillation, cardioversion, and pacing. Circulation. 2010;122(18)(suppl 3):S706-S719. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
