

Surgical Excision of Heterotopic Ossification Leads to Re-Emergence of Mesenchymal Stem Cell Populations Responsible for Recurrence
- PMID: 28297577
- PMCID: PMC5442786
- DOI: 10.5966/sctm.2015-0365
Surgical Excision of Heterotopic Ossification Leads to Re-Emergence of Mesenchymal Stem Cell Populations Responsible for Recurrence
Abstract
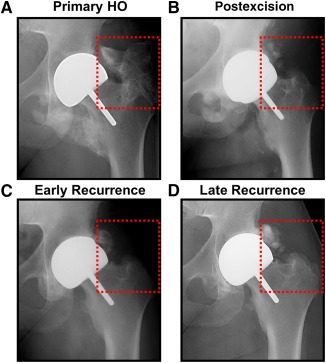
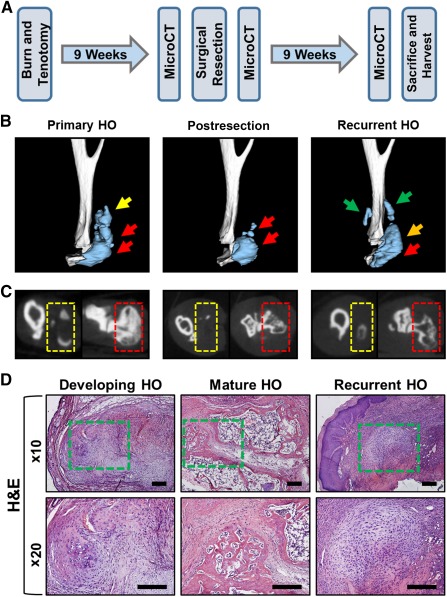
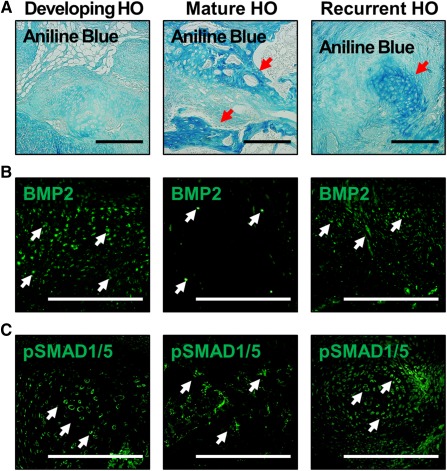
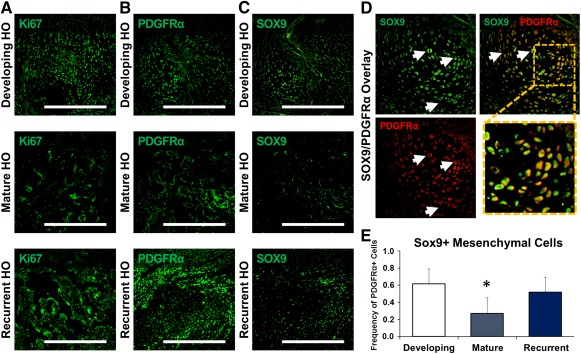
Trauma-induced heterotopic ossification (HO) occurs after severe musculoskeletal injuries and burns, and presents a significant barrier to patient rehabilitation. Interestingly, the incidence of HO significantly increases with repeated operations and after resection of previous HO. Treatment of established heterotopic ossification is challenging because surgical excision is often incomplete, with evidence of persistent heterotopic bone. As a result, patients may continue to report the signs or symptoms of HO, including chronic pain, nonhealing wounds, and joint restriction. In this study, we designed a model of recurrent HO that occurs after surgical excision of mature HO in a mouse model of hind-limb Achilles' tendon transection with dorsal burn injury. We first demonstrated that key signaling mediators of HO, including bone morphogenetic protein signaling, are diminished in mature bone. However, upon surgical excision, we have noted upregulation of downstream mediators of osteogenic differentiation, including pSMAD 1/5. Additionally, surgical excision resulted in re-emergence of a mesenchymal cell population marked by expression of platelet-derived growth factor receptor-α (PDGFRα) and present in the initial developing HO lesion but absent in mature HO. In the recurrent lesion, these PDGFRα+ mesenchymal cells are also highly proliferative, similar to the initial developing HO lesion. These findings indicate that surgical excision of HO results in recurrence through similar mesenchymal cell populations and signaling mechanisms that are present in the initial developing HO lesion. These results are consistent with findings in patients that new foci of ectopic bone can develop in excision sites and are likely related to de novo formation rather than extension of unresected bone. Stem Cells Translational Medicine 2017;6:799-806.
Keywords: Bone; Chondrogenesis; Extremity trauma; Heterotopic ossification; Mesenchymal stem cell; Tissue regeneration.
© 2016 The Authors Stem Cells Translational Medicine published by Wiley Periodicals, Inc. on behalf of AlphaMed Press.
Figures

References
-
- Levi B, Jayakumar P, Giladi A et al. Risk factors for the development of heterotopic ossification in seriously burned adults: A National Institute on Disability, Independent Living and Rehabilitation Research burn model system database analysis. J Trauma Acute Care Surg 2015;79:870–876. - PMC - PubMed
-
- Potter BK, Forsberg JA, Davis TA et al. Heterotopic ossification following combat‐related trauma. J Bone Joint Surg Am 2010;92 (suppl): 274–89. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
