

Plasmablast Response to Primary Rhesus Cytomegalovirus (CMV) Infection in a Monkey Model of Congenital CMV Transmission
- PMID: 28298291
- PMCID: PMC5424243
- DOI: 10.1128/CVI.00510-16
Plasmablast Response to Primary Rhesus Cytomegalovirus (CMV) Infection in a Monkey Model of Congenital CMV Transmission
Abstract
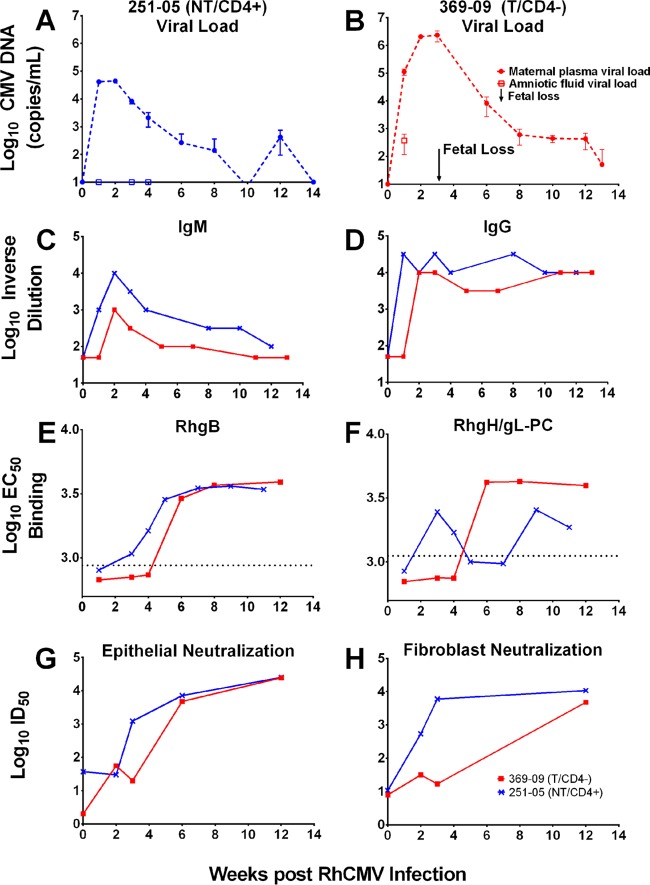
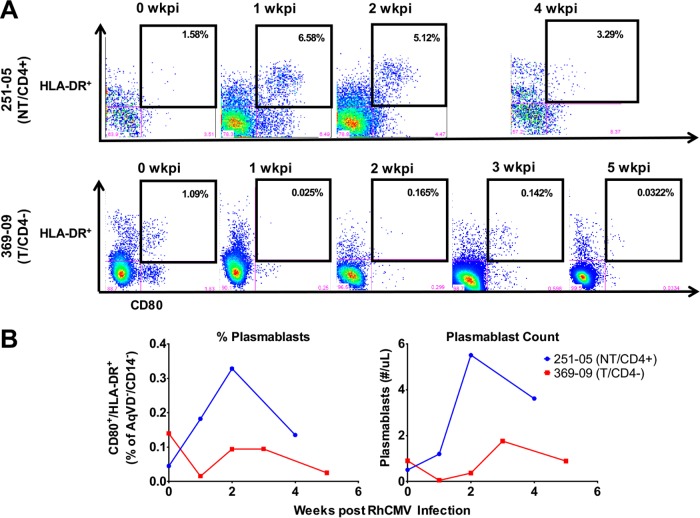
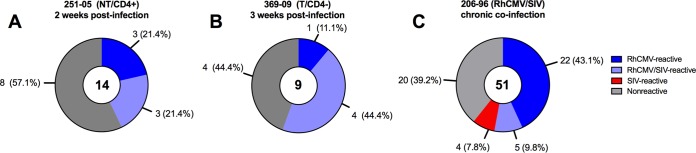
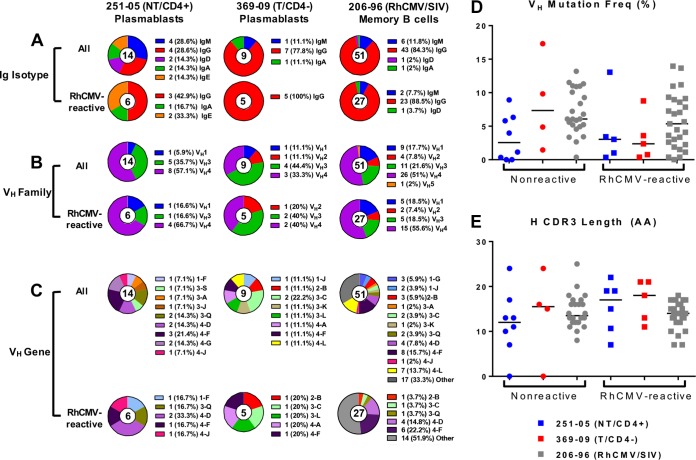
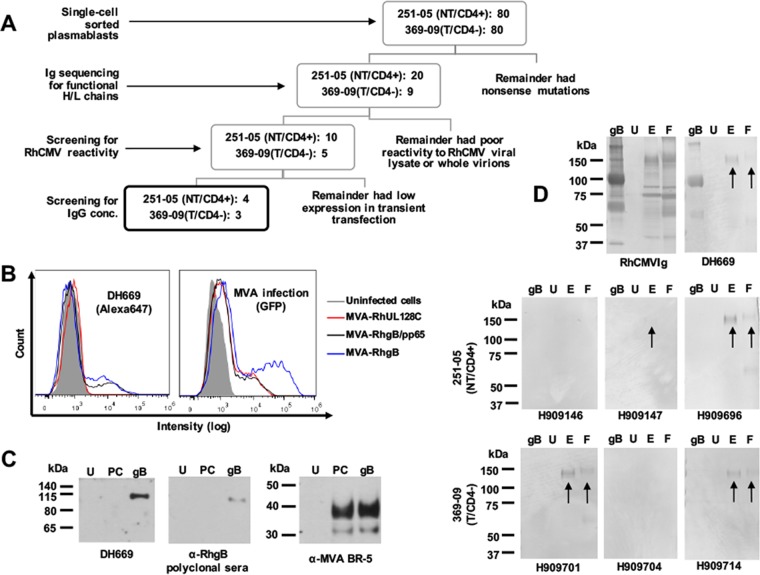
Human cytomegalovirus (HCMV) is the most common congenital infection worldwide and the leading infectious cause of neurologic deficits and hearing loss in newborns. Development of a maternal HCMV vaccine to prevent vertical virus transmission is a high priority, yet protective maternal immune responses following acute infection are poorly understood. To characterize the maternal humoral immune response to primary CMV infection, we investigated the plasmablast and early antibody repertoire using a nonhuman primate model with two acutely rhesus CMV (RhCMV)-infected animals-a CD4+ T cell-depleted dam that experienced fetal loss shortly after vertical RhCMV transmission and an immunocompetent dam that did not transmit RhCMV to her infant. Compared to the CD4+ T cell-depleted dam that experienced fetal loss, the immunocompetent, nontransmitting dam had a more rapid and robust plasmablast response that produced a high proportion of RhCMV-reactive antibodies, including the first identified monoclonal antibody specific for soluble and membrane-associated RhCMV envelope glycoprotein B (gB). Additionally, we noted that plasmablast RhCMV-specific antibodies had variable gene usage and maturation similar to those observed in a monkey chronically coinfected with simian immunodeficiency virus (SIV) and RhCMV. This study reveals characteristics of the early maternal RhCMV-specific humoral immune responses to primary RhCMV infection in rhesus monkeys and may contribute to a future understanding of what antibody responses should be targeted by a vaccine to eliminate congenital HCMV transmission. Furthermore, the identification of an RhCMV gB-specific monoclonal antibody underscores the possibility of modeling future HCMV vaccine strategies in this nonhuman primate model.
Keywords: congenital cytomegalovirus; nonhuman primates; vaccine.
Copyright © 2017 American Society for Microbiology.
Figures
Similar articles
-
Maternal CD4+ T cells protect against severe congenital cytomegalovirus disease in a novel nonhuman primate model of placental cytomegalovirus transmission.Proc Natl Acad Sci U S A. 2015 Nov 3;112(44):13645-50. doi: 10.1073/pnas.1511526112. Epub 2015 Oct 19. Proc Natl Acad Sci U S A. 2015. PMID: 26483473 Free PMC article.
-
Relationship of maternal cytomegalovirus-specific antibody responses and viral load to vertical transmission risk following primary maternal infection in a rhesus macaque model.PLoS Pathog. 2023 Oct 23;19(10):e1011378. doi: 10.1371/journal.ppat.1011378. eCollection 2023 Oct. PLoS Pathog. 2023. PMID: 37871009 Free PMC article.
-
Protective effect of pre-existing natural immunity in a nonhuman primate reinfection model of congenital cytomegalovirus infection.bioRxiv [Preprint]. 2023 Apr 10:2023.04.10.536057. doi: 10.1101/2023.04.10.536057. bioRxiv. 2023. Update in: PLoS Pathog. 2023 Oct 5;19(10):e1011646. doi: 10.1371/journal.ppat.1011646. PMID: 37090643 Free PMC article. Updated. Preprint.
-
Maternal immune correlates of protection against placental transmission of cytomegalovirus.Placenta. 2017 Dec;60 Suppl 1(Suppl 1):S73-S79. doi: 10.1016/j.placenta.2017.04.011. Epub 2017 Apr 20. Placenta. 2017. PMID: 28456432 Free PMC article. Review.
-
Rhesus cytomegalovirus a nonhuman primate model for the study of human cytomegalovirus.Adv Virus Res. 2008;72:207-26. doi: 10.1016/S0065-3527(08)00405-3. Adv Virus Res. 2008. PMID: 19081492 Review.
Cited by
-
A comparison of unamplified and massively multiplexed PCR amplification for murine antibody repertoire sequencing.FASEB Bioadv. 2019 Jan;1(1):6-17. Epub 2018 Aug 30. FASEB Bioadv. 2019. PMID: 30740592 Free PMC article.
-
Immune Correlates of Protection Against Human Cytomegalovirus Acquisition, Replication, and Disease.J Infect Dis. 2020 Mar 5;221(Suppl 1):S45-S59. doi: 10.1093/infdis/jiz428. J Infect Dis. 2020. PMID: 32134477 Free PMC article.
-
Prior dengue virus serotype 3 infection modulates subsequent plasmablast responses to Zika virus infection in rhesus macaques.mBio. 2024 Mar 13;15(3):e0316023. doi: 10.1128/mbio.03160-23. Epub 2024 Feb 13. mBio. 2024. PMID: 38349142 Free PMC article.
-
Animal Models of Congenital Cytomegalovirus Transmission: Implications for Vaccine Development.J Infect Dis. 2020 Mar 5;221(Suppl 1):S60-S73. doi: 10.1093/infdis/jiz484. J Infect Dis. 2020. PMID: 32134481 Free PMC article. Review.
-
Rhesus monkeys for a nonhuman primate model of cytomegalovirus infections.Curr Opin Virol. 2017 Aug;25:126-133. doi: 10.1016/j.coviro.2017.08.005. Epub 2017 Sep 6. Curr Opin Virol. 2017. PMID: 28888133 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
