

Diagnosis of chronic thromboembolic pulmonary hypertension
- PMID: 28298387
- PMCID: PMC9488918
- DOI: 10.1183/16000617.0108-2016
Diagnosis of chronic thromboembolic pulmonary hypertension
Abstract
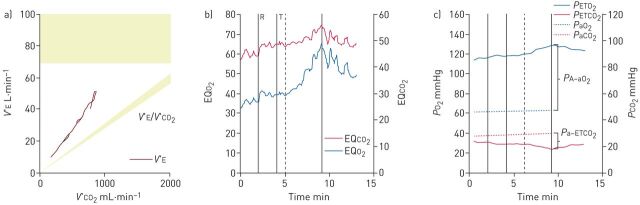
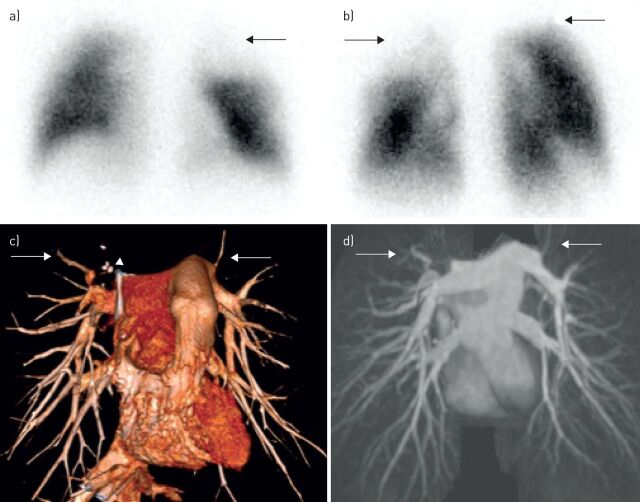
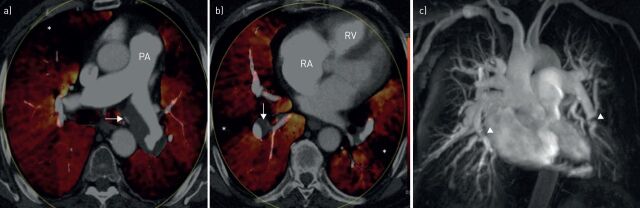
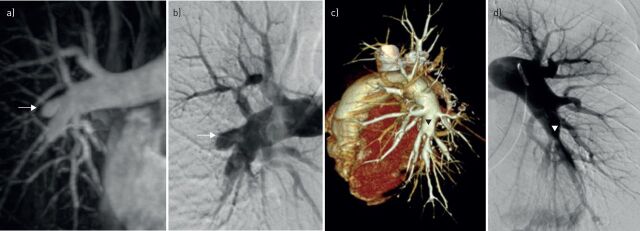
Chronic thromboembolic pulmonary hypertension (CTEPH) is the only potentially curable form of pulmonary hypertension. Rapid and accurate diagnosis is pivotal for successful treatment. Clinical signs and symptoms can be nonspecific and risk factors such as history of venous thromboembolism may not always be present. Echocardiography is the recommended first diagnostic step. Cardiopulmonary exercise testing is a complementary tool that can help to identify patients with milder abnormalities and chronic thromboembolic disease, triggering the need for further investigation. Ventilation/perfusion (V'/Q') scintigraphy is the imaging methodology of choice to exclude CTEPH. Single photon emission computed tomography V'/Q' is gaining popularity over planar imaging. Assessment of pulmonary haemodynamics by right heart catheterisation is mandatory, although there is increasing interest in noninvasive haemodynamic evaluation. Despite the status of digital subtraction angiography as the gold standard, techniques such as computed tomography (CT) and magnetic resonance imaging are increasingly used for characterising the pulmonary vasculature and assessment of operability. Promising new tools include dual-energy CT, combination of rotational angiography and cone beam CT, and positron emission tomography. These innovative procedures not only minimise misdiagnosis, but also provide additional vascular information relevant to treatment planning. Further research is needed to determine how these modalities will fit into the diagnostic algorithm for CTEPH.
Copyright ©ERS 2017.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside this article at
Figures
Similar articles
-
Diagnostic advances and opportunities in chronic thromboembolic pulmonary hypertension.Eur Respir Rev. 2015 Jun;24(136):253-62. doi: 10.1183/16000617.00000915. Eur Respir Rev. 2015. PMID: 26028637 Free PMC article. Review.
-
Chronic Thromboembolic Pulmonary Hypertension: Pearls and Pitfalls of Diagnosis.Methodist Debakey Cardiovasc J. 2016 Oct-Dec;12(4):199-204. doi: 10.14797/mdcj-12-4-199. Methodist Debakey Cardiovasc J. 2016. PMID: 28289494 Free PMC article. Review.
-
Chronic thromboembolic pulmonary hypertension (CTEPH) - potential role of multidetector-row CT (MD-CT) and MR imaging in the diagnosis and differential diagnosis of the disease.Rofo. 2014 Aug;186(8):751-61. doi: 10.1055/s-0034-1366425. Epub 2014 Apr 22. Rofo. 2014. PMID: 24756429 Review.
-
Imaging techniques in chronic thromboembolic pulmonary hypertension.Curr Opin Pulm Med. 2013 Sep;19(5):562-74. doi: 10.1097/MCP.0b013e3283645a00. Curr Opin Pulm Med. 2013. PMID: 23880705 Review.
-
Ventilation-perfusion scintigraphy is more sensitive than multidetector CTPA in detecting chronic thromboembolic pulmonary disease as a treatable cause of pulmonary hypertension.J Nucl Med. 2007 May;48(5):680-4. doi: 10.2967/jnumed.106.039438. J Nucl Med. 2007. PMID: 17475953
Cited by
-
Peripheral Arterial Stiffness in Acute Pulmonary Embolism and Pulmonary Hypertension at Short-Term Follow-Up.J Clin Med. 2021 Jul 6;10(14):3008. doi: 10.3390/jcm10143008. J Clin Med. 2021. PMID: 34300176 Free PMC article.
-
Contemporary treatment of right ventricular failure.JHLT Open. 2024 Dec 30;7:100203. doi: 10.1016/j.jhlto.2024.100203. eCollection 2025 Feb. JHLT Open. 2024. PMID: 40144829 Free PMC article. Review.
-
Interventional Imaging Roadmap to Successful Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension.J Soc Cardiovasc Angiogr Interv. 2022 Aug 12;1(6):100429. doi: 10.1016/j.jscai.2022.100429. eCollection 2022 Nov-Dec. J Soc Cardiovasc Angiogr Interv. 2022. PMID: 39132377 Free PMC article. Review.
-
EANM guideline for ventilation/perfusion single-photon emission computed tomography (SPECT) for diagnosis of pulmonary embolism and beyond.Eur J Nucl Med Mol Imaging. 2019 Nov;46(12):2429-2451. doi: 10.1007/s00259-019-04450-0. Epub 2019 Aug 13. Eur J Nucl Med Mol Imaging. 2019. PMID: 31410539 Free PMC article.
-
Chronic thromboembolic pulmonary hypertension in Saudi Arabia: preliminary results from the SAUDIPH registry.ERJ Open Res. 2020 May 11;6(2):00218-2019. doi: 10.1183/23120541.00218-2019. eCollection 2020 Apr. ERJ Open Res. 2020. PMID: 32420315 Free PMC article.
References
-
- Fedullo P, Kerr KM, Kim NH, et al. . Chronic thromboembolic pulmonary hypertension. Am J Respir Crit Care Med 2011; 183: 1605–1613. - PubMed
-
- Dentali F, Donadini M, Gianni M, et al. . Incidence of chronic pulmonary hypertension in patients with previous pulmonary embolism. Thromb Res 2009; 124: 256–258. - PubMed
-
- Poli D, Grifoni E, Antonucci E, et al. . Incidence of recurrent venous thromboembolism and of chronic thromboembolic pulmonary hypertension in patients after a first episode of pulmonary embolism. J Thromb Thrombolysis 2010; 30: 294–299. - PubMed
-
- Pepke-Zaba J, Delcroix M, Lang I, et al. . Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international prospective registry. Circulation 2011; 124: 1973–1981. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical