

Clinical Manifestations, Treatment, and Diagnosis of Tropheryma whipplei Infections
- PMID: 28298472
- PMCID: PMC5355640
- DOI: 10.1128/CMR.00033-16
Clinical Manifestations, Treatment, and Diagnosis of Tropheryma whipplei Infections
Abstract
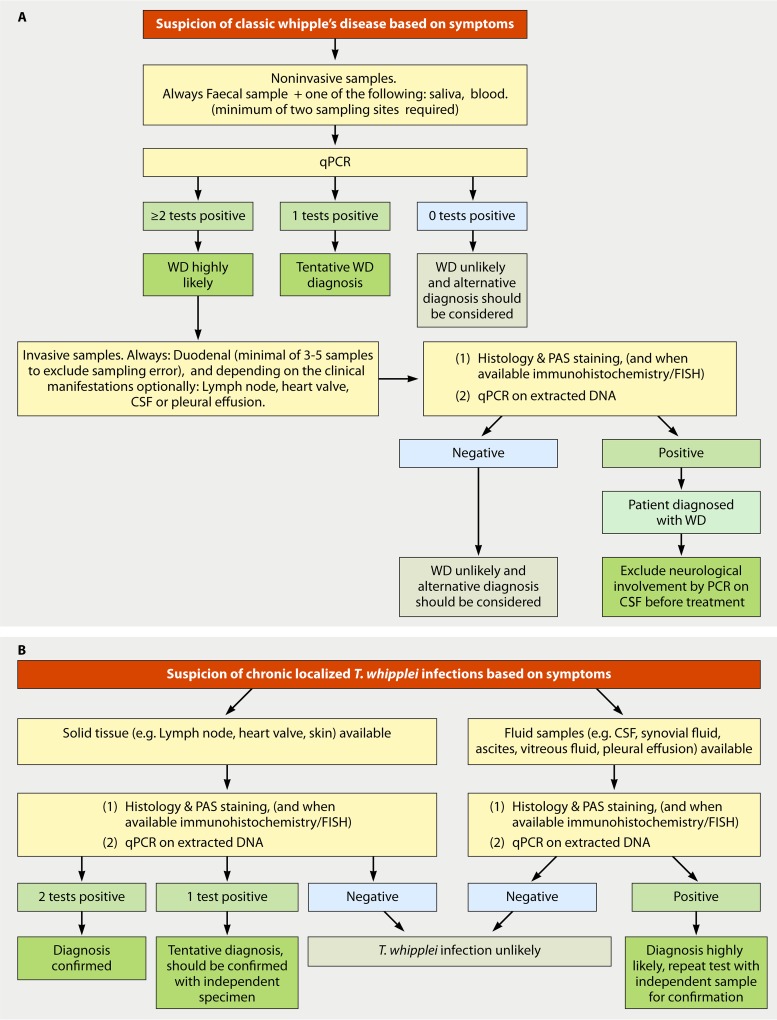
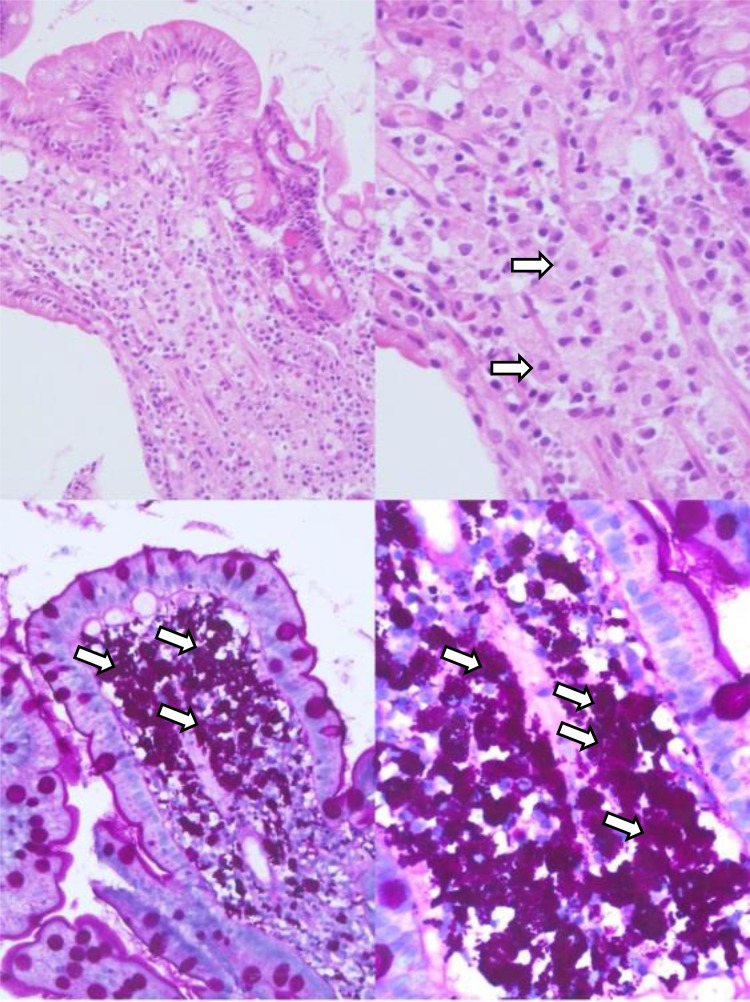
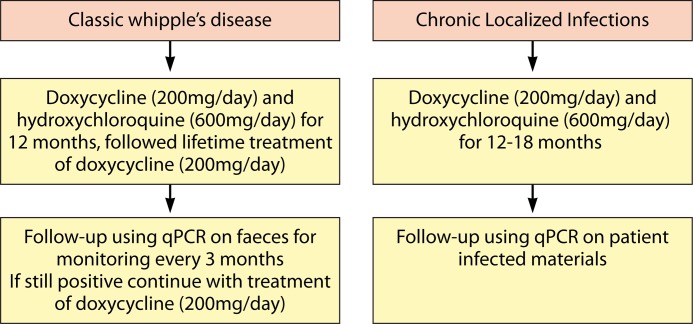
Whipple's disease is a rare infectious disease that can be fatal if left untreated. The disease is caused by infection with Tropheryma whipplei, a bacterium that may be more common than was initially assumed. Most patients present with nonspecific symptoms, and as routine cultivation of the bacterium is not feasible, it is difficult to diagnose this infection. On the other hand, due to the generic symptoms, infection with this bacterium is actually quite often in the differential diagnosis. The gold standard for diagnosis used to be periodic acid-Schiff (PAS) staining of duodenal biopsy specimens, but PAS staining has a poor specificity and sensitivity. The development of molecular techniques has resulted in more convenient methods for detecting T. whipplei infections, and this has greatly improved the diagnosis of this often missed infection. In addition, the molecular detection of T. whipplei has resulted in an increase in knowledge about its pathogenicity, and this review gives an overview of the new insights in epidemiology, pathogenesis, clinical manifestations, diagnosis, and treatment of Tropheryma whipplei infections.
Keywords: PCR; Tropheryma whipplei; Whipple's disease; antibiotics; clinical manifestations; histopathology; therapy.
Copyright © 2017 American Society for Microbiology.
Figures



References
-
- Whipple GH. 1907. A hitherto undescribed disease characterized anatomically by deposits of fat and fatty acids in the intestinal and mesenteric lymphatic tissues. Bull Johns Hopkins Hosp 18:382–393.
-
- Paulley JW. 1952. A case of Whipple's disease (intestinal lipodystrophy). Gastroenterology 22:128–133. - PubMed
-
- Yardley JH, Hendrix TR. 1961. Combined electron and light microscopy in Whipple's disease. Demonstration of “bacillary bodies” in the intestine. Bull Johns Hopkins Hosp 109:80–98. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
