

In vivo feasibility of real-time MR-US fusion imaging lumbar facet joint injections
- PMID: 28298941
- PMCID: PMC5334272
- DOI: 10.1007/s40477-016-0233-2
In vivo feasibility of real-time MR-US fusion imaging lumbar facet joint injections
Abstract
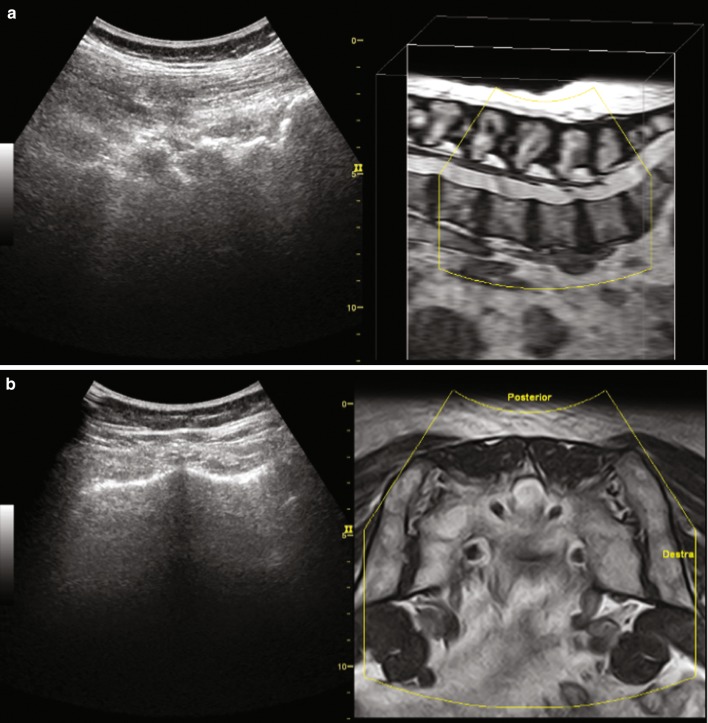
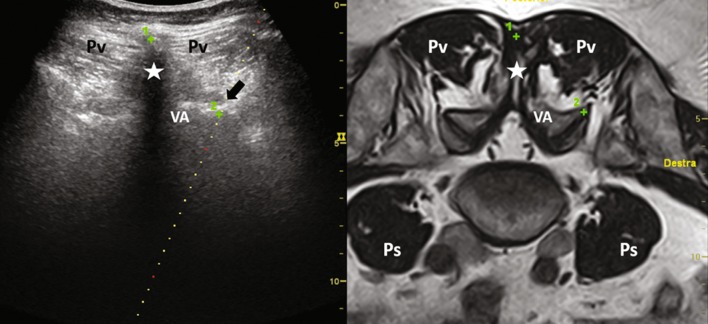
Objectives: Traditionally, facet joint injections (FJI) are performed under fluoroscopic or computed tomography (CT) guidance, mainly due to the deep anatomical location and the presence of bony landmarks. Fusion imaging technology, which couples the ultrasound scan with the corresponding CT or magnetic resonance (MR) image obtained from the diagnostic examination and reformatted in real time according to the ultrasound scanning plane, allows to combine the panoramic view and the elevated anatomical detail of MR or CT with the ease of use of ultrasound without patient exposure to ionizing radiation.
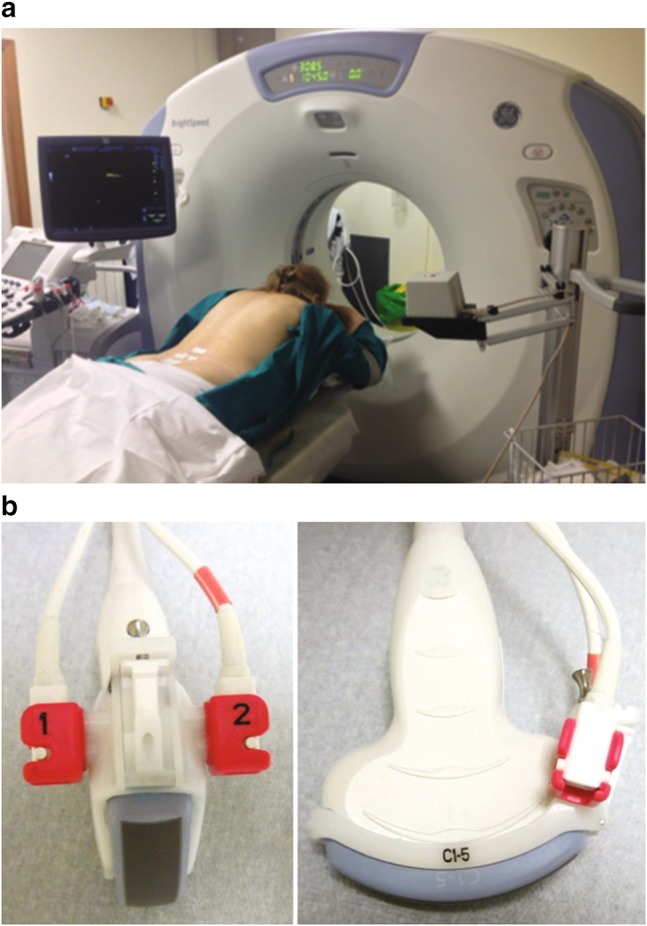
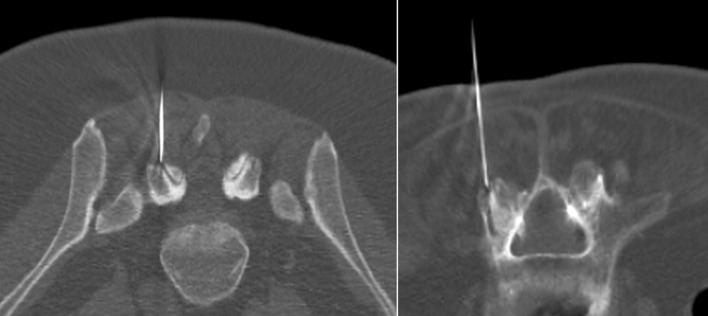
Methods: Thirty eight patients (24 females; mean age ± SD: 64 ± 9 years) received MR fusion-assisted ultrasound-guided FJI of 1 ml of a mixture of local anaesthetic and corticosteroid using a ultrasound machine (Logiq E9, GE Healthcare) equipped with a GPS-enhanced fusion imaging technology which couples real-time B-mode images with those of the previous recent diagnostic MR examination. Low-dose CT needle positioning confirmation was performed in the first 28 patients. Patients' pain was recorded using a visual analogue scale (VAS), at baseline and at 2, 4 and 8 weeks.
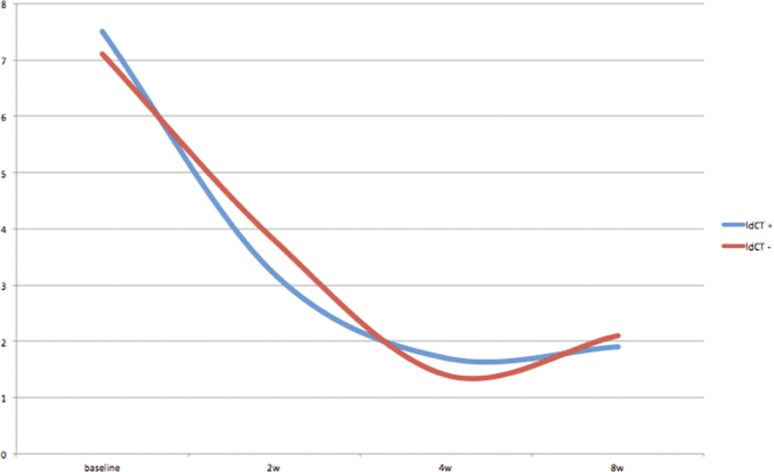
Results: All fusion imaging-guided injections were performed successfully. Out of 112, 96 FJI had optimal intra-articular needle positioning (accuracy: 85.7%). Patients VAS significantly decreases after the procedure with no differences among who received CT needle positioning control and who did not receive it. No major complications were observed.
Conclusions: Ultrasound needle guidance with MR fusion assistance allows for safe and effective injection of degenerative facet joint disease.
Obiettivi: Tradizionalmente, le iniezioni delle faccette articolari (FJI) sono state eseguite sotto guida fluoroscopica o tomografia computerizzata (TC), principalmente a causa della posizione anatomica profonda e la presenza di reperi ossei. L’imaging di fusione permette di accoppiare le immagine ecografiche con quelle TC o di risonanza magnetica (RM) corrispondenti, ottenute da un precedente esame diagnostico e riformattate in tempo reale in base al piano di scansione ecografico. Questa tecnica permette di coniugare la visione panoramica e l’elevato dettaglio anatomico della RM o TC con la praticità della guida ecografica senza ulteriore esposizione del paziente a radiazioni ionizzanti.
Metodi: Trentotto pazienti (24 femmine, età media ± DS: 64 ± 9 anni) hanno ricevuto FJI guidata da fusione ecografia-RM di 1 ml di una miscela di anestetico locale e corticosteroide utilizzando una apparecchiatura ecografica (Logiq E9, GE Healthcare) dotata di tecnologia fusion. Nei primi 28 pazienti il posizionamento dell’ago è stato confermato mediante esame TC a bassa dose. Il dolore dei pazienti è stato registrato utilizzando una scala analogica visiva (VAS), al tempo 0 e dopo 2, 4 e 8 settimane.
Risultati: Tutte le iniezioni fusion guidate sono state eseguite con successo. In 96 su 112 iniezioni è stato raggiunto lo spazio intra-articolare (precisione: 85,7%). La VAS è diminuita significativamente dopo la procedura in tutti i pazienti, senza differenze tra chi ha ricevuto il controllo CT del posizionamento degli aghi e chi non lo ha ricevuto. Non sono state osservate complicanze maggiori.
Conclusioni: L’iniezione fusion ecografia-RM guidata delle faccette articolari artrosiche rappresenta una opzione terapeutica sicura ed efficace.
Obiettivi: Tradizionalmente, le iniezioni delle faccette articolari (FJI) sono state eseguite sotto guida fluoroscopica o tomografia computerizzata (TC), principalmente a causa della posizione anatomica profonda e la presenza di reperi ossei. L’imaging di fusione permette di accoppiare le immagine ecografiche con quelle TC o di risonanza magnetica (RM) corrispondenti, ottenute da un precedente esame diagnostico e riformattate in tempo reale in base al piano di scansione ecografico. Questa tecnica permette di coniugare la visione panoramica e l’elevato dettaglio anatomico della RM o TC con la praticità della guida ecografica senza ulteriore esposizione del paziente a radiazioni ionizzanti.
Metodi: Trentotto pazienti (24 femmine, età media ± DS: 64 ± 9 anni) hanno ricevuto FJI guidata da fusione ecografia-RM di 1 ml di una miscela di anestetico locale e corticosteroide utilizzando una apparecchiatura ecografica (Logiq E9, GE Healthcare) dotata di tecnologia fusion. Nei primi 28 pazienti il posizionamento dell’ago è stato confermato mediante esame TC a bassa dose. Il dolore dei pazienti è stato registrato utilizzando una scala analogica visiva (VAS), al tempo 0 e dopo 2, 4 e 8 settimane.
Risultati: Tutte le iniezioni fusion guidate sono state eseguite con successo. In 96 su 112 iniezioni è stato raggiunto lo spazio intra-articolare (precisione: 85,7%). La VAS è diminuita significativamente dopo la procedura in tutti i pazienti, senza differenze tra chi ha ricevuto il controllo CT del posizionamento degli aghi e chi non lo ha ricevuto. Non sono state osservate complicanze maggiori.
Conclusioni: L’iniezione fusion ecografia-RM guidata delle faccette articolari artrosiche rappresenta una opzione terapeutica sicura ed efficace.
Keywords: Facet joint; Fusion imaging; Injection; Magnetic resonance; Ultrasound.
Conflict of interest statement
Conflict of interest
The authors have no conflict of interest to disclose.
Ethical standard
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. The present study was approved by the Institutional review board.
Informed consent
Informed patients’ consent was obtained for the present study.
Figures

References
-
- Lewinnek GE, Warfield CA. Facet joint degeneration as a cause of low back pain. Clin Orthop Relat Res. 1986;213:216–222. - PubMed
-
- Boswell MV, Colson JD, Sehgal N, Dunbar EE, Epter R. A systematic review of therapeutic facet joint interventions in chronic spinal pain. Pain Physician. 2007;10(1):229–253. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
