

Cardiac Events After Radiation Therapy: Combined Analysis of Prospective Multicenter Trials for Locally Advanced Non-Small-Cell Lung Cancer
- PMID: 28301264
- PMCID: PMC5455464
- DOI: 10.1200/JCO.2016.71.6142
Cardiac Events After Radiation Therapy: Combined Analysis of Prospective Multicenter Trials for Locally Advanced Non-Small-Cell Lung Cancer
Abstract
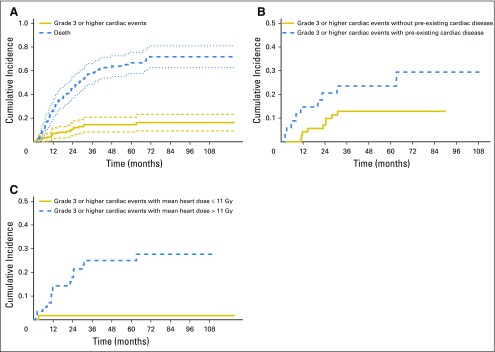
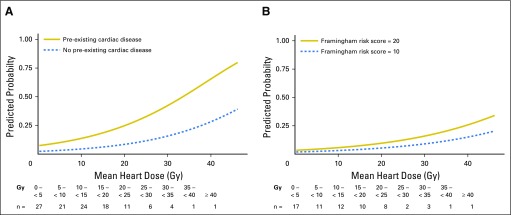
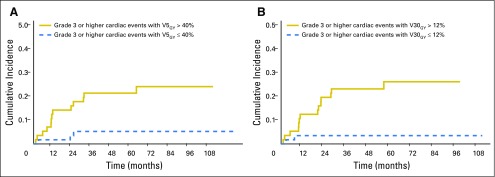
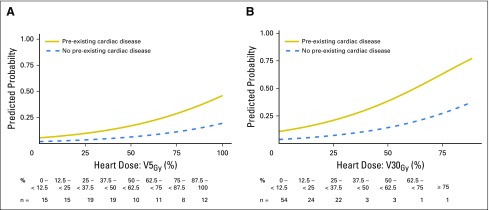
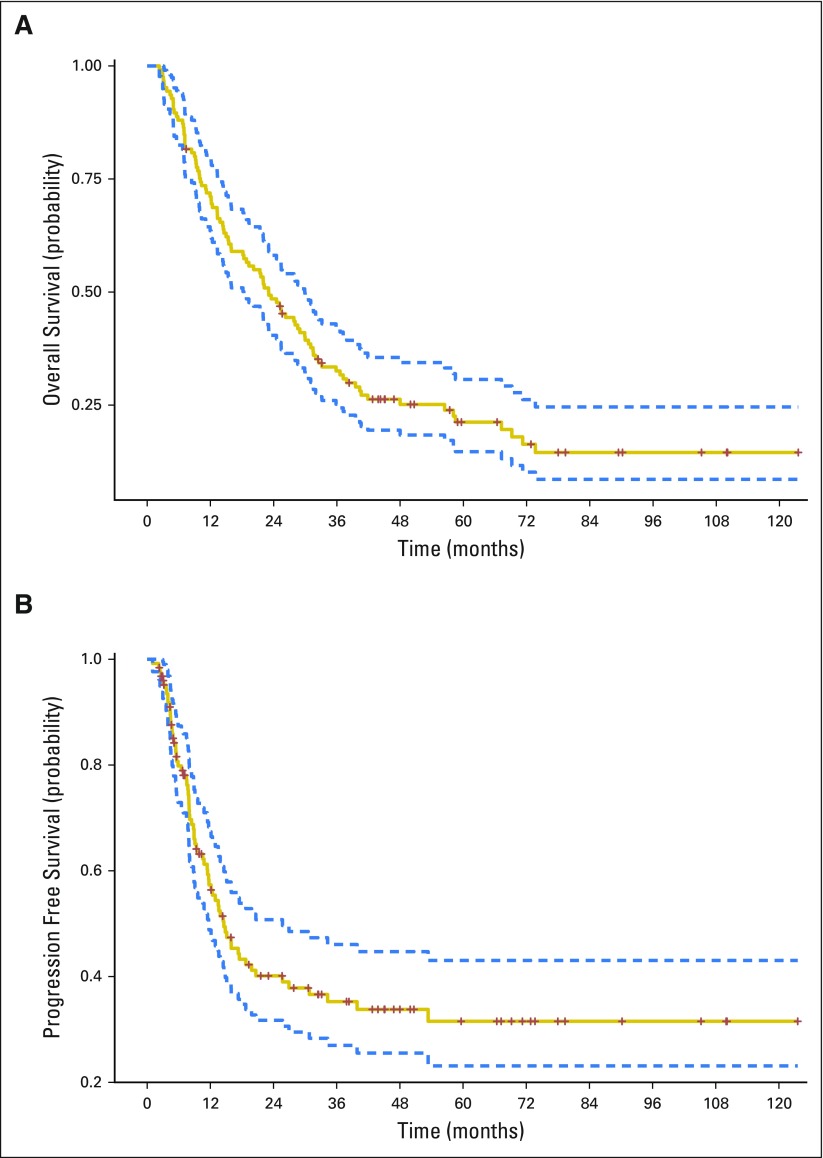
Purpose Radiation therapy is a critical component in the care of patients with non-small-cell lung cancer (NSCLC), yet cardiac injury after treatment is a significant concern. Therefore, we wished to elucidate the incidence of cardiac events and their relationship to radiation dose to the heart. Patients and Materials Study eligibility criteria included patients with stage II to III NSCLC treated on one of four prospective radiation therapy trials at two centers from 2004 to 2013. All cardiac events were reviewed and graded per Common Terminology Criteria for Adverse Events (v4.03). The primary end point was the development of a grade ≥ 3 cardiac event. Results In all, 125 patients met eligibility criteria; median follow-up was 51 months for surviving patients. Median prescription dose was 70 Gy, 84% received concurrent chemotherapy, and 27% had pre-existing cardiac disease. Nineteen patients had a grade ≥ 3 cardiac event at a median of 11 months (interquartile range, 6 to 24 months), and 24-month cumulative incidence was 11% (95% CI, 5% to 16%). On multivariable analysis (MVA), pre-existing cardiac disease (hazard ratio [HR], 2.96; 95% CI, 1.07 to 8.21; P = .04) and mean heart dose (HR, 1.07/Gy; 95% CI, 1.02 to 1.13/Gy; P = .01) were significantly associated with grade ≥ 3 cardiac events. Analyzed as time-dependent variables on MVA analysis, both disease progression (HR, 2.15; 95% CI, 1.54 to 3.00) and grade ≥ 3 cardiac events (HR, 1.76; 95% CI, 1.04 to 2.99) were associated with decreased overall survival. However, disease progression (n = 71) was more common than grade ≥ 3 cardiac events (n = 19). Conclusion The 24-month cumulative incidence of grade ≥ 3 cardiac events exceeded 10% among patients with locally advanced NSCLC treated with definitive radiation. Pre-existing cardiac disease and higher mean heart dose were significantly associated with higher cardiac event rates. Caution should be used with cardiac dose to minimize risk of radiation-associated injury. However, cardiac risks should be balanced against tumor control, given the unfavorable prognosis associated with disease progression.
Figures
Comment in
-
Locally Advanced Lung Cancer: Is It Time to Take Cardiac Protection Seriously in Radiation Planning?Int J Radiat Oncol Biol Phys. 2018 Apr 1;100(5):1091-1094. doi: 10.1016/j.ijrobp.2017.09.044. Int J Radiat Oncol Biol Phys. 2018. PMID: 29722650 No abstract available.
References
-
- Perez CA, Stanley K, Rubin P, et al. A prospective randomized study of various irradiation doses and fractionation schedules in the treatment of inoperable non-oat-cell carcinoma of the lung: Preliminary report by the Radiation Therapy Oncology Group. Cancer. 1980;45:2744–2753. - PubMed
-
- Aupérin A, Le Péchoux C, Rolland E, et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol. 2010;28:2181–2190. - PubMed
-
- Machtay M, Bae K, Movsas B, et al: Higher biologically effective dose of radiotherapy is associated with improved outcomes for locally advanced non-small cell lung carcinoma treated with chemoradiation: An analysis of the Radiation Therapy Oncology Group. Int J Radiat Oncol Biol Phys 82:425-434, 2012 - PMC - PubMed
-
- Martel MK, Ten Haken RK, Hazuka MB, et al. Estimation of tumor control probability model parameters from 3-D dose distributions of non-small cell lung cancer patients. Lung Cancer. 1999;24:31–37. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
