

Clinical laboratories collaborate to resolve differences in variant interpretations submitted to ClinVar
- PMID: 28301460
- PMCID: PMC5600649
- DOI: 10.1038/gim.2017.14
Clinical laboratories collaborate to resolve differences in variant interpretations submitted to ClinVar
Abstract
Purpose: Data sharing through ClinVar offers a unique opportunity to identify interpretation differences between laboratories. As part of a ClinGen initiative, four clinical laboratories (Ambry, GeneDx, Partners Healthcare Laboratory for Molecular Medicine, and University of Chicago Genetic Services Laboratory) collaborated to identify the basis of interpretation differences and to investigate if data sharing and reassessment resolve interpretation differences by analyzing a subset of variants.
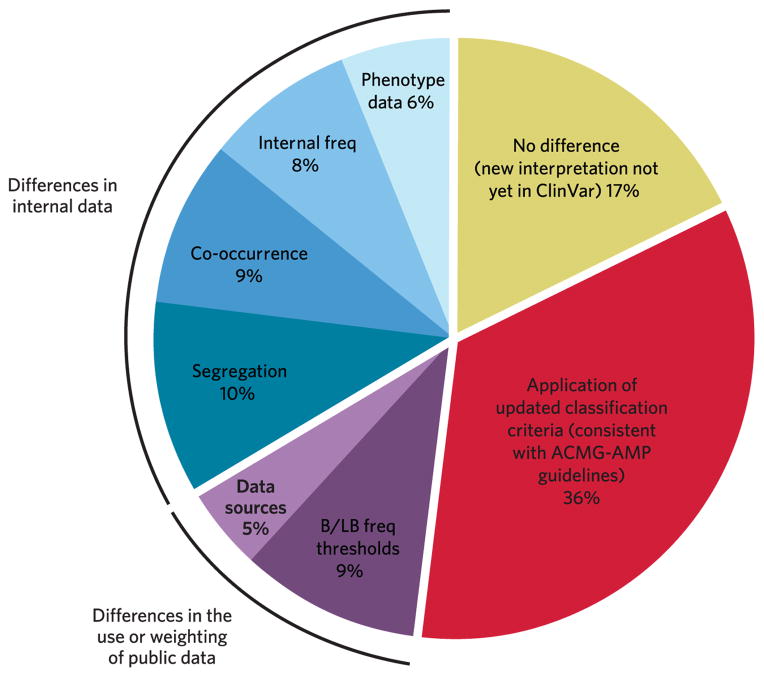
Methods: ClinVar variants with submissions from at least two of the four participating laboratories were compared. For a subset of identified differences, laboratories documented the basis for discordance, shared internal data, independently reassessed with the American College of Medical Genetics and Genomics-Association for Molecular Pathology (ACMG-AMP) guidelines, and then compared interpretations.
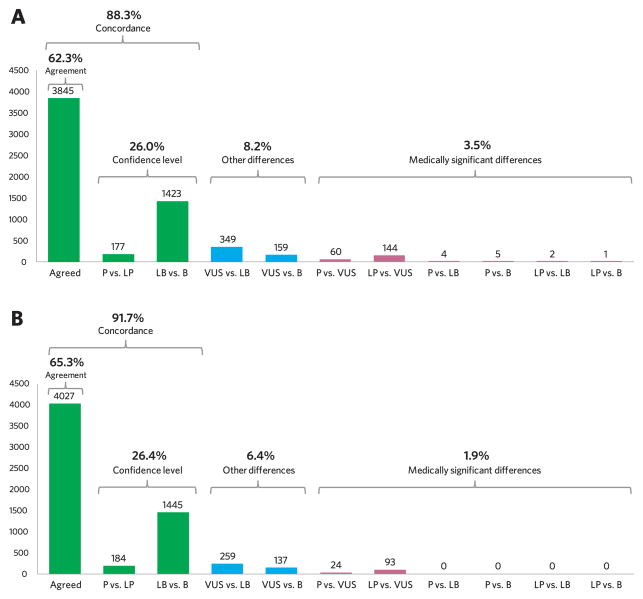
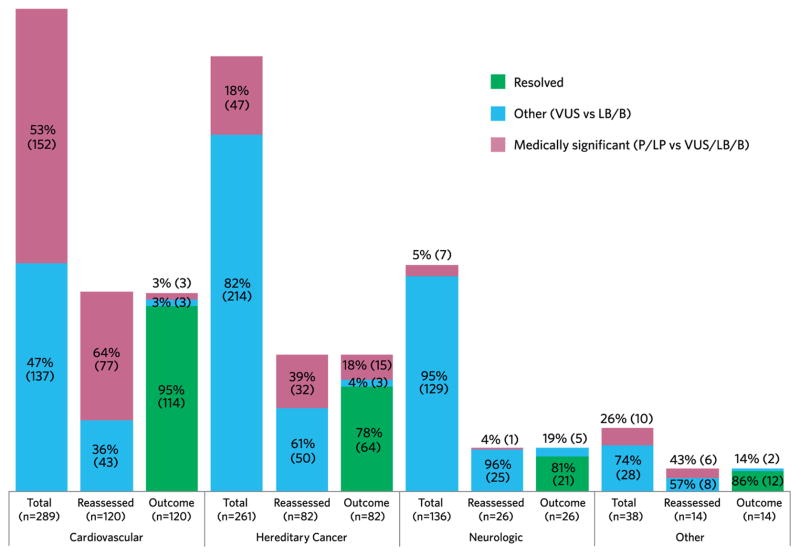
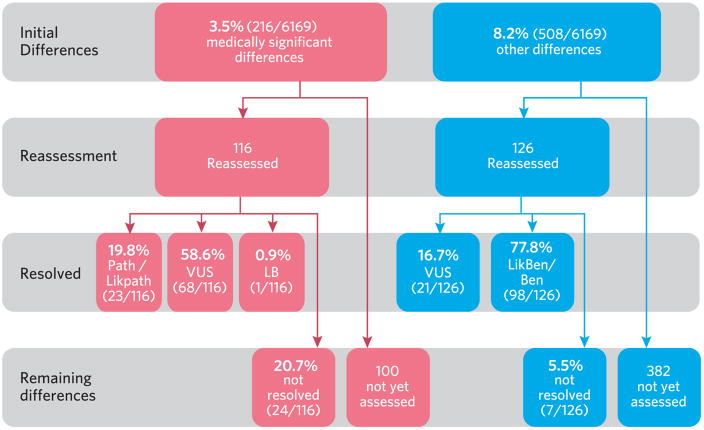
Results: At least two of the participating laboratories interpreted 6,169 variants in ClinVar, of which 88.3% were initially concordant. Laboratories reassessed 242/724 initially discordant variants, of which 87.2% (211) were resolved by reassessment with current criteria and/or internal data sharing; 12.8% (31) of reassessed variants remained discordant owing to differences in the application of the ACMG-AMP guidelines.
Conclusion: Participating laboratories increased their overall concordance from 88.3 to 91.7%, indicating that sharing variant interpretations in ClinVar-thereby allowing identification of differences and motivation to resolve those differences-is critical to moving toward more consistent variant interpretations.Genet Med advance online publication 09 March 2017.
Conflict of interest statement
All authors are clinical service providers and are employed by laboratories which offer fee-based clinical sequencing. This employment is noted in the author affiliations. All authors declare no additional conflicts of interest beyond their employment affiliation.
Figures
References
-
- Yorczyk A, Robinson LS, Ross TS. Use of panel tests in place of single gene tests in the cancer genetics clinic. Clin Genet. 2015;88(3):278–282. - PubMed
-
- Pepin MG, Murray ML, Bailey S, et al. The challenge of comprehensive and consistent sequence variant interpretation between clinical laboratories. Genet Med. 2016;18(1):20–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
