

Spectral detector CT for cardiovascular applications
- PMID: 28302592
- PMCID: PMC5410998
- DOI: 10.5152/dir.2016.16255
Spectral detector CT for cardiovascular applications
Abstract
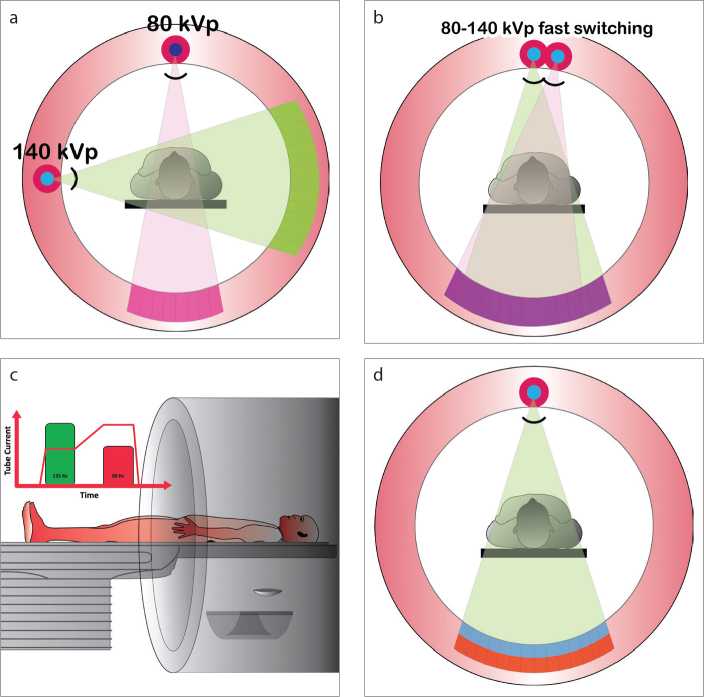
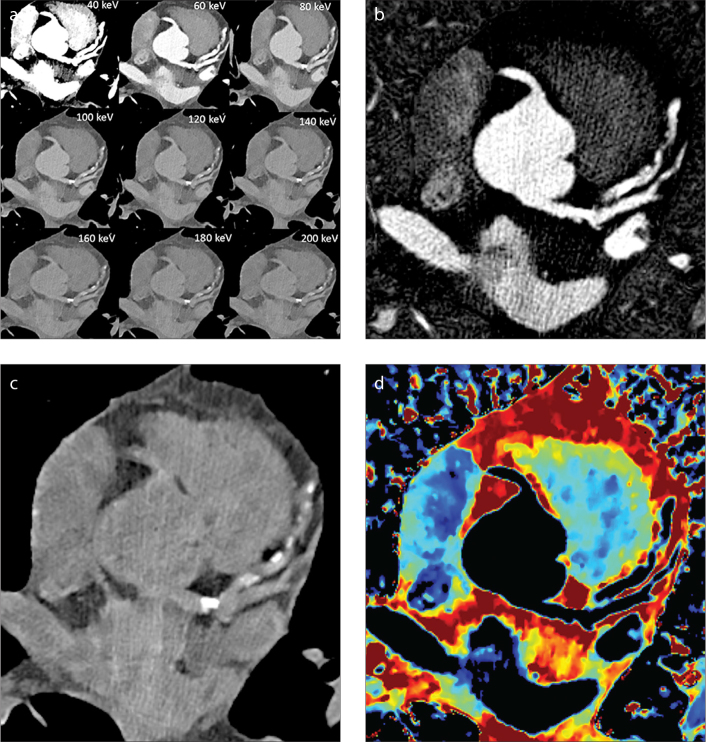
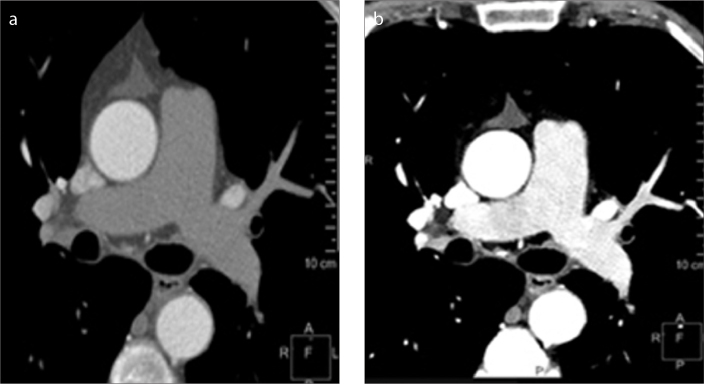
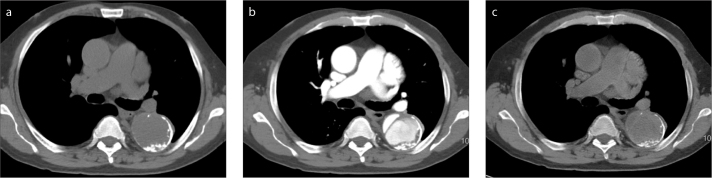
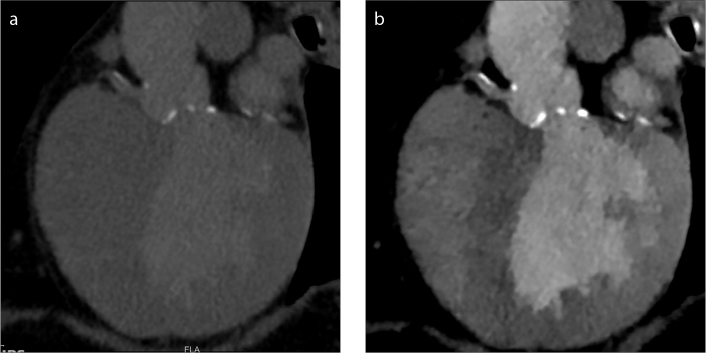
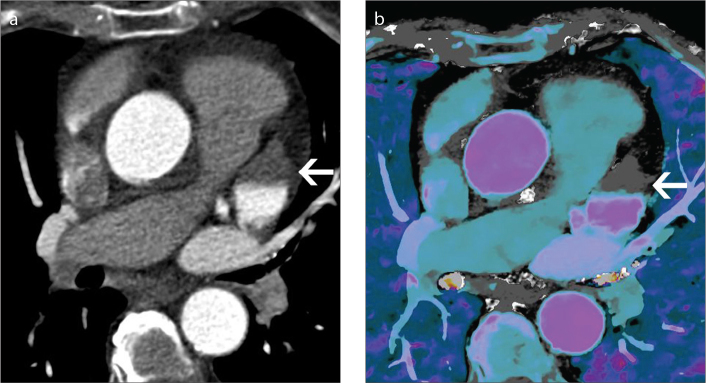
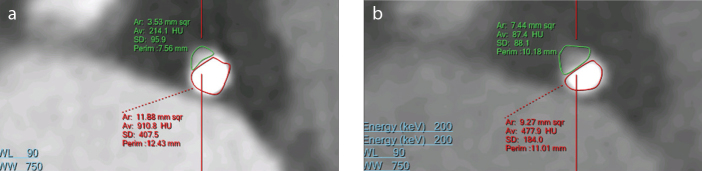
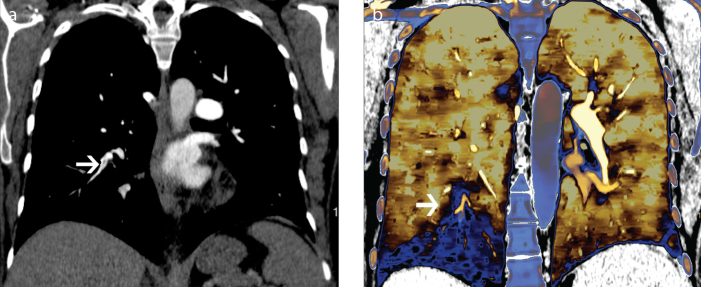
Spectral detector computed tomography (SDCT) is a novel technology that uses two layers of detectors to simultaneously collect low and high energy data. Spectral data is used to generate conventional polyenergetic images as well as dedicated spectral images including virtual monoenergetic and material composition (iodine-only, virtual unenhanced, effective atomic number) images. This paper provides an overview of SDCT technology and a description of some spectral image types. The potential utility of SDCT for cardiovascular imaging and the impact of this new technology on radiation and contrast dose are discussed through presentation of initial patient studies performed on a SDCT scanner. The value of SDCT for salvaging suboptimal studies including those with poor contrast-enhancement or beam hardening artifacts through retrospective reconstruction of spectral data is discussed. Additionally, examples of specific benefits for the evaluation of aortic disease, imaging before transcatheter aortic valve implantation, evaluation of pulmonary veins pre- and post-pulmonary radiofrequency ablation, evaluation of coronary artery lumen, assessment of myocardial perfusion, detection of pulmonary embolism, and characterization of incidental findings are presented.
Conflict of interest statement
Prabhakar Rajiah has received institutional research support and honoraria from Philips Healthcare. Suhny Abbara has received institutional research support from Philips Healthcare. Sandra Halliburton is a Philips Healthcare employee.
Figures
References
-
- Johnson TRC. Dual-energy CT: General principles. Am J Roentgenol. 2012;199:S3–8. https://doi.org/10.2214/AJR.12.9116. - DOI - PubMed
-
- Goodsitt MM, Christodoulou EG, Larson SC. Accuracies of the synthesized monochromatic CT numbers and effective atomic numbers obtained with a rapid kVp switching dual energy CT scanner. Med Phys. 2011;38:2222–2232. https://doi.org/10.1118/1.3567509. - DOI - PubMed
-
- Alvarez RE, Macovski A. Energy-selective reconstructions in X-ray computerized tomography. Phys Med Biol. 1976;21:633–644. https://doi.org/10.1088/0031-9155/21/5/002. - DOI - PubMed
-
- Vlahos I, Chung R, Nair A, Morgan R. Dual-energy CT: vascular applications. Am J Roentgenol. 2012;199:S87–97. https://doi.org/10.2214/AJR.12.9114. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
