

Heart Failure in Pediatric Patients With Congenital Heart Disease
- PMID: 28302743
- PMCID: PMC5391045
- DOI: 10.1161/CIRCRESAHA.116.308996
Heart Failure in Pediatric Patients With Congenital Heart Disease
Abstract
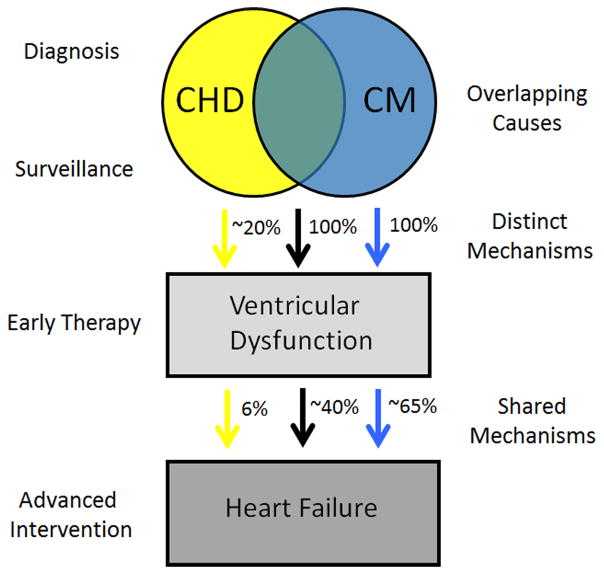
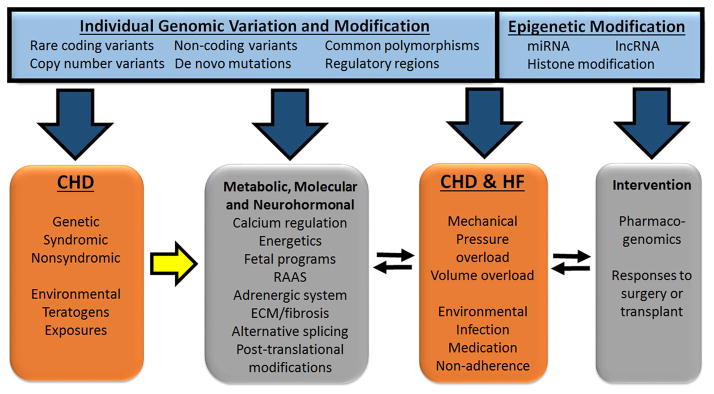
Heart failure (HF) is a complex clinical syndrome resulting from diverse primary and secondary causes and shared pathways of disease progression, correlating with substantial mortality, morbidity, and cost. HF in children is most commonly attributable to coexistent congenital heart disease, with different risks depending on the specific type of malformation. Current management and therapy for HF in children are extrapolated from treatment approaches in adults. This review discusses the causes, epidemiology, and manifestations of HF in children with congenital heart disease and presents the clinical, genetic, and molecular characteristics that are similar or distinct from adult HF. The objective of this review is to provide a framework for understanding rapidly increasing genetic and molecular information in the challenging context of detailed phenotyping. We review clinical and translational research studies of HF in congenital heart disease including at the genome, transcriptome, and epigenetic levels. Unresolved issues and directions for future study are presented.
Keywords: cardiovascular malformation; genetics; mutation; single ventricle; stem cell; ventricular dysfunction.
© 2017 American Heart Association, Inc.
Figures
References
-
- Kirk R, Dipchand AI, Rosenthal DN, Addonizio L, Burch M, Chrisant M, Dubin A, Everitt M, Gajarski R, Mertens L, Miyamoto S, Morales D, Pahl E, Shaddy R, Towbin J, Weintraub R. The international society for heart and lung transplantation guidelines for the management of pediatric heart failure: Executive summary [corrected] J Heart Lung Transplant. 2014;33:888–909. - PubMed
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW American College of Cardiology F, American Heart A. 2009 focused update incorporated into the acc/aha 2005 guidelines for the diagnosis and management of heart failure in adults a report of the american college of cardiology foundation/american heart association task force on practice guidelines developed in collaboration with the international society for heart and lung transplantation. Journal of the American College of Cardiology. 2009;53:e1–e90. - PubMed
-
- Ross RD, Daniels SR, Schwartz DC, Hannon DW, Shukla R, Kaplan S. Plasma norepinephrine levels in infants and children with congestive heart failure. The American journal of cardiology. 1987;59:911–914. - PubMed
-
- Connolly D, Rutkowski M, Auslender M, Artman M. The new york university pediatric heart failure index: A new method of quantifying chronic heart failure severity in children. J Pediatr. 2001;138:644–648. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
